By Saddam Mazar, M. Idrees Shah, Shahbaz Khan Panhwar, Syed Ata ur Rahman, Syeda Laibah Ali
AFFLIATIONS:
Department of Orthopedics and Spine Surgery, Dr. Ziauddin University Hospital, Karachi, Pakistan.
DOI: https://doi.org/10.36283/PJMD11-3/008
ORCID iD: 0000-0002-9426-5100
How to cite: Mazar S, SI, Panhwar SK, Rahman SA, Ali SL. Functional Outcomes of Close Reduction With K-wires Vs Open Reduction and Internal Fixation in Distal Radius Fractures. Pak J Med Dent. 2022;11(3):44-50. doi: 10.36283/PJMD11-3/008
Background: Radius and/or ulna fractures are frequent which encounter higher emergency room visits. Despite high incidence, proper management between closed reduction and internal fixation (CRIF) with K-wires and open reduction and internal fixation (ORIF) with anatomical Volar locking plate, remains debatable. This study aimed to compare the functional outcomes between the two management protocols.
Methods: A total of 118 patients with distal radius fractures were treated operatively, at Dr. Ziauddin University Hospital Karachi, from January 2017 to October 2020. Out of these, 29 patients (24.6%) were treated with CRIF and 89 patients (75.4%) with ORIF. The functional outcomes of both groups were assessed through disabilities of arm, shoulder and hand (DASH) scores at 3 and 6 months. functional outcomes were assessed through a t-test, p-value <0.05 was considered significant.
Results: The male to female ratio was 2.5:1, with an average age of 40.9 years. The Arbeitsgemeinschaft für Osteosynthesefragen (AO) 23-B type injury was observed in 29 (24.6%) patients. The mean DASH score among the ORIF group and CRIF group at 3 months was 43.03 and 46.19 (p <0.007) respectively. Whereas the DASH score of the ORIF and CRIF group at 6 months was 41.35 and 44.70 (p <0.007) respectively. Both groups at 6 months of management reported 33 (28%) patients with complete satisfaction, however, the return to work in the ORIF group was found highly significant (p=0.00).
Conclusion: Open reduction and internal fixation with the distal radius locking compression plate produce functionally improved outcomes compared to K-wires for displaced distal radius fractures.
Keywords: Radius, Bone Wires; Open Fracture Reduction; Fracture Fixation.
The 640,000 radius and/or ulna fractures were reported in the United States alone, in 2001, accounting for nearly 1.5 percent of all emergency room visits. In the pediatrics and elderly populations, distal radius fractures account for 25% and 18% of all fractures, respectively1,2. As a result of increasing average life expectancy, distal radius articular fractures are reliably increasing3. Because of increased functional demand by elderly patients and short duration of functional rehabilitation as compared to non-operative cast immobilization leading to stiffness of wrist and fingers, a rising increase in surgical versus non-operative treatment of displaced articular fractures has recently been described3.
Non-displaced simple fractures are usually treated without surgery with a plaster cast. Because they heal in an unfavorable anatomical position, unstable fractures are commonly treated surgically4. Closed reduction and percutaneous K-wire fixation, fixation with volar or dorsal plates (locking or nonlocking), bridge plating, use of an external fixator, or a combination of these treatments are surgical and nonsurgical management options for patients with distal radius fractures1,2. Although the optimum treatment decision is dependent on the fracture characteristics (open/closed, un-displaced/displaced, extra-/intra-articular), there is just a small body of high-quality evidence to support it. The American Academy of Orthopedic Surgeons (AAOS) provided 29 recommendations in their clinical practice guidelines for distal radius fracture; none of these recommendations obtained a satisfactory grade due to the poor quality of the evidence1.
External fixation and Kirschner-wire stabilization have been linked to an increased risk of infection in several studies2. Patients with high demands may benefit from open reduction with locking volar plates, even if functional outcomes in older individuals with low needs are satisfactory despite the presence of a deformity2.
The introduction of locking plates with locking screws opened new surgical possibilities for fracture fixation and stability, even with comminuted fractures and osteoporosis4. On the volar side of the wrist, the radial artery is radially retracted, and the fracture is exposed, reduced, and set with a locking plate and screws utilizing the FCR technique. Early wrist range of motion is crucial for a successful postoperative recovery with volar plating. In any scenario, if standard locking plate application principles are not followed, there is a considerable risk of consequences such as median nerve palsy, tendon irritation, and tendon rupture4. There have been favorable outcomes of distal radius volar locking plate as compared to CRIF with K-wires group because of earlier mobilization3.
In a study published in 2018, it was found that Closed reduction and percutaneous pinning (CRPP) was an effective tool for recovering radiographic parameters following carefully selected types A and C distal radius fractures and that most patients had a good or exceptional range of wrist mobility after treatment with CRPP5. The objective was to determine the functional outcomes in patients with displaced distal radius fractures treated with CRIF with K-wires with ORIF with distal radius Volar locking plate in this study.
In this study, 118 patients, who sustained Distal Radius Fractures, were included and retrospectively analyzed, with 89 of them receiving Open Reduction and Internal Fixation (ORIF) and 29 receiving CRIF (with K-wires), and were managed at Dr. Ziauddin University Hospital Karachi from January 2017 to October 2020. The study included patients of all ages, genders, and races who matched the inclusion criteria.
The inclusion criteria included all patients with >18 years of age, sustaining isolated distal radius fracture with >15° lateral displacement and>5mm radial shortening on the frontal plane, and fractures classified as B, C1-C2 type (Simple articular fractures) in AO classification. While exclusion criteria consisted of all open fractures and compromised neurovascular state, polytrauma, A and C3 type fractures types in AO, ipsilateral upper extremity fracture (Floating elbow) and bilateral wrist fractures.
In the ORIF group, the treatment protocol followed with FCR approach, reduction and internal fixation with angular stable plate and functional rehabilitation 15 days following surgery; while CRIF with K-wires followed Closed reduction and percutaneous K-wire fixation, 2-3 K-wires implanted from distal to the proximal region of fracture engaging opposing cortex and one K-wire for distal stability of radio-ulnar joint, if necessary, further stabilized in a brachio-metacarpal plaster cast. The wires and cast were removed after 6 weeks, followed by functional rehabilitation.
For patients that were surgically managed with Open Reduction and Internal Fixation (ORIF), the flexor carpi radialis (FCR) approach for Distal Radius Fracture was utilized, and the surgeons were familiar with the implants used. The patient selection for ORIF and K-Wire was decided considering the fracture pattern, patient’s medical and clinical history and presenting status, adequacy of closed reduction and surgeon choice. All the patients’ clinical and radiological findings were documented both before and after surgery. The study used anteroposterior and lateral X-ray scans of the wrist as radiographic examinations.
In a few patients undergoing ORIF, a wrist splint was applied post-operatively, which was removed two weeks later during the follow-up visit. Concomitantly, the splint applied with K-wires was removed at the period of 6 weeks along with the K-wires. Metal staple sutures were used in cases with ORIF and were removed after 2 weeks. Antibiotics were used for three doses perioperatively and analgesics were advised considering each patient. The DASH score was used to calculate the Functional Outcomes (at 3 and 6 months of follow-up). A t-test was used to compare the functional outcomes of the two groups, and it was done on SPSS version 23.0.
A total of 118 patients were managed for Distal Radius Articular Fractures. Of these 34(28.8 %) were females and 84 (71.2 %) were males with an M: F ratio of 2.5:1. The average age of the participants was around 40.9. The right-hand dominancy was found in 94 patients (79.7 %) while left-hand dominant patients were 24 (20.3%). There were 33 (28.0%) patients with reported tobacco smoking. The patients with desk jobs were 88 (74.6%) while field workers were 30 (25.4%). It was observed to have AO 23-B in 29 patients (24.6%), AO 23-C1 to be 52 patients (44.1%) and AO 23-C2 fractures in 37 patients (31.4 %) (Table 1 and Figure 1).
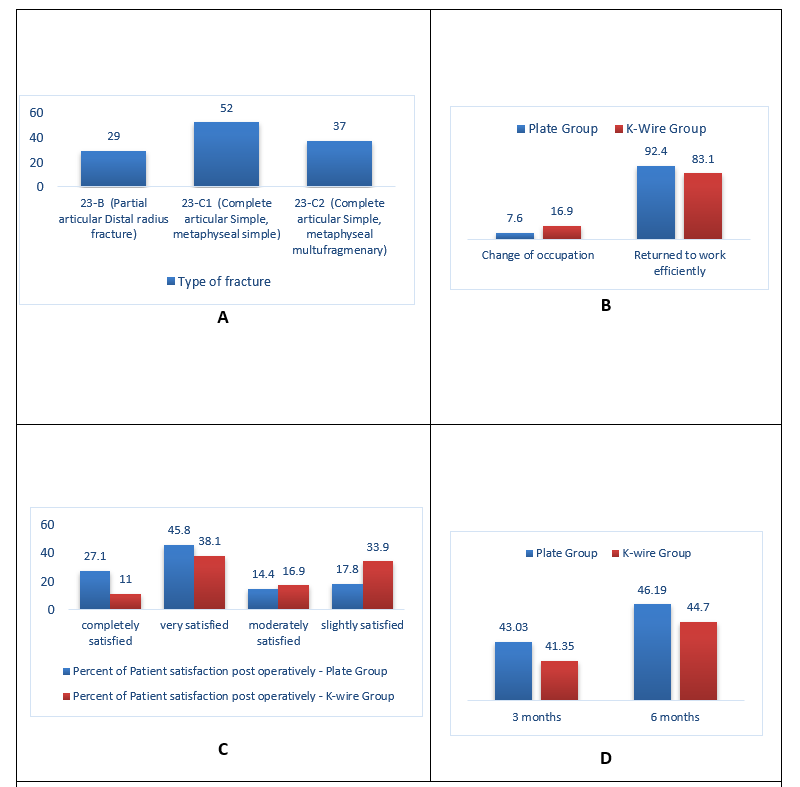
Figure 1 (A-D): Comparison of mean DASH scores between plate and K-wire group at 3 and 6 months (p =0.007).
Table 1: Distribution of variable “return to work” in comparison to the type of fracture.
| Variables | Types of Fracture | |||
| 23-B (Partial Articular Distal Radius Fracture) | 23-C1 (Complete Articular Simple, Metaphyseal Simple) | 23-C2 (Complete Articular Simple, Metaphyseal Multi-Fragmentary) | ||
| Counts | ||||
| Plate Group | Change of occupation | 3 | 4 | 2 |
| Returned to work effectively | 26 | 48 | 35 | |
| K-Wire Group | Change of occupation | 7 | 4 | 9 |
| Returned to work effectively | 22 | 48 | 28 | |
A total of 29 patients (24.6%) were treated with CRIF while the remaining 89 patients (75.4%) had surgical interventions (ORIF) performed (p =0.000). Among the ORIF group, the mean value for the DASH Score was found to be 43.03 and 46.19 at 3 months and 6 months, respectively, with 26 out of 89 (29.2%) with a DASH Score of equal and more than 55, who reported a much better result, while the mean DASH Score among CRIF group was found to be 41.35 and 44.70 at 3 months and 6 months, respectively (p =0.007). Of the patients who returned to perform their work 109 (92.4%) while those who changed their occupation were 9 (7.6%). A significant association was found between occupation and type of fracture patterns (p =0.067). The patient reported satisfaction was found as 33 (28%) with complete satisfaction with the management, 54 (45.8%) were moderately satisfied while 14 (11.9%) were slightly satisfied, for both groups at 6 months of management (Table 2). Among patients treated with ORIF, 92.4% returned to work efficiently and 7.6 % of patients changed their occupations, while 83.1% returned to work efficiently and 16.9% changed their occupations in the K-Wire group.
Table 2: Comparison of different variables between the two groups.
| Variables Comparison | Treatment Protocol – Plate Group | Treatment Protocol – Plate/K-Wire Group | |||
| Treatment Protocol – K-Wire Group | Total | p-Value | |||
| Counts | |||||
| Gender | Male | 66 | 18 | 84 | 0.215 |
| Female | 23 | 11 | 34 | ||
| Dominant Working Hand | Right hand dominant | 73 | 21 | 94 | 0.268 |
| left hand dominant | 16 | 8 | 24 | ||
| Tobacco Smoking | non-smoker | 62 | 14 | 76 | 0.132 |
| Smoker | 20 | 13 | 33 | ||
| casual/social smoker | 7 | 2 | 9 | ||
| Type of Occupation | desk job | 70 | 18 | 88 | 0.076 |
| fieldwork | 19 | 11 | 30 | ||
| Type of Fracture | 23-B (Partial articular Distal radius fracture) | 0 | 29 | 29 | 0.000 |
| 23-C1 (Complete articular Simple, metaphyseal simple) | 52 | 0 | 52 | ||
| 23-C2 (Complete articular Simple, metaphyseal multi-fragmentary) | 37 | 0 | 37 | ||
| Return to Work | change of occupation | 6 | 3 | 9 | 0.000 |
| returned to work effectively | 83 | 26 | 109 | ||
| Patient satisfaction post operatively | slightly satisfied | 13 | 1 | 14 | 0.000 |
| moderately satisfied | 12 | 5 | 17 | ||
| very satisfied | 39 | 15 | 54 | ||
| completely satisfied | 25 | 8 | 33 | ||
In comparison to Kirschner-wire (K-wire) closed fixation, open reduction and internal fixation (ORIF) with volar locking plate yielded much better outcomes. The DASH score was used to quantitatively examine the data in this study, which aimed to compare the functional outcomes of the two procedures. In the current study, the male to female ratio was 2.47:1, indicating that males were found to be more prevalent in the current study data. This differs from a previous study that found the M: F ratio to be 1:3 in the past10. In the United States, a woman’s lifetime chance of suffering a distal radius fracture is estimated to be 15%, whereas men’s risk is only 2% 11. Because this study was conducted in a low-resource situation, the authors speculate that environmental factors may have influenced the male-to-female ratio of fracture survivors.
The volar locking plate (VLP) and Kirschner wire/pin fixations are the most popular surgical fixation techniques for distal radius fractures, notably in the United Kingdom10,12. Both are effective treatments for dorsally displaced, unstable, extra-articular, or simple intra-articular distal radius fractures13. To keep the fracture in the proper anatomical position, K-wires are introduced through the skin over the dorsal face of the distal radius and into the bone. Through an incision made across the volar (palm) area of the wrist, the locking plate is secured to the bone with fixed angle locking screws. To stabilize the most complex fractures, a volar fixed-angle plate must support the dorsal, central, and volar aspects of the subchondral bone14,15. Even though external K-wire fixation is a common technique for treating unstable distal radius fractures, a study published in 2019 found that VLP fixation outperformed external K-wire fixation in terms of wrist mobility, ulnar variance correction, and articular congruence improvement16,17. Wire fixation is insufficient in complex intraarticular type fractures of the distal radius when compared to VLP because it causes more volar tilt loss and arthritic changes in the postoperative period18. Other significant differences in functional outcomes have been discovered in previous studies, such as the volar locking plate group having better alignment restoration in terms of volar tilt and radial length19. Furthermore, the anatomical reduction was significantly more likely to be preserved in the plating group20.
The main theoretical benefits of plating internal fixation for distal radius fractures could be the early functional recovery seen in this study, as well as a previous comparative study that found that using ORIF with a volar fixed-angle implant resulted in stable fixation of the distal articular fragments, allowing for early postsurgical wrist motion21. Another comprehensive study published in 2015 found that volar locking plates for displaced distal radius fractures in adults have better DASH scores at 3- and 12-month follow-up when compared to K-wires and external fixation, as well as a lower overall incidence of problems, lower infection rates, and much better flexion-extension motion22,23. Furthermore, ORIF is associated with superior functional outcomes, which is advantageous for patients who require a faster return to function following surgery, particularly in present study case where we had 88 (74.6%) patients with a desk job and 30 (25.4%) patients who were field workers13. The average age in this study conducted at Ziauddin hospital was 40.9, but findings suggest that ORIF with plates is also an effective treatment alternative in patients above 60 years of age which adds to its advantages24.
There are some limitations to the current study. Firstly, the small sample size increases the chances of unreliability in the results, like the research conducted in the past with a small sample13,25,26. Second, due to the small number of trials, we did not conduct any follow-up outcomes to examine long-term effects, as no significant differences between the two types of treatment have been detected in long-term follow-up studies completed to date10,27. Lastly, the cost-effectiveness of both the procedures was not taken into consideration. K wire fixation, comparatively, is an inexpensive procedure28-30. To the authors’ knowledge, very few studies have been conducted locally comparing the two procedures and thus, the research can serve as a preliminary study. To further look at the effectiveness of this intervention, more thorough research should be done for patient satisfaction with larger sample size and more randomized control trials are needed to obtain better results.
In conclusion, the main aim of the intervention is to secure and maintain anatomic reduction of joint surface to achieve better levels of patient satisfaction and better functional outcomes, along with ensuring minimal complications. In the current study, open reduction with internal fixation yielded better results.
Regardless of the age or gender of the patients, the candidates who were successfully surgically managed with Volar plating for fractures of the distal radius reported a much better functional outcome, in comparison to those patients who were treated with K-wires.
The authors would like to thank the Ziauddin Hospital for the facilitation and smooth conduction of the research.
The authors declared no conflict of interest.
The study was approved by the ethics review committee of the Ziauddin University with the reference code: 4351021SMORT.
Informed consent was taken from patients. Patient identity was not disclosed at any point during the research.
Idea conceptualization, writing, data collection and data analysis were done by SM. MIS also assisted in the idea conceptualization and reviewed the manuscript. SKP had written the manuscript and performed the data analysis. SAR did the data collection and SLA assisted in paper writing and data collection
- Azad A, Kang HP, Alluri RK, Vakhshori V, Kay HF, Ghiassi A. Epidemiological and treatment trends of distal radius fractures across multiple age groups. J Wrist Surg. 2019;8(04):305-311. doi: 10.1055/s-0039-1685205
- Chaudhry H, Kleinlugtenbelt YV, Mundi R, Ristevski B, Goslings JC, Bhandari M. Are volar locking plates superior to percutaneous K-wires for distal radius fractures? A meta-analysis. Clin Orthop Relat Res. 2015;473(9):3017-3027. doi: 10.1007/s11999-015-4347-1
- Ju JH, Jin GZ, Li GX, Hu HY, Hou RX. Comparison of treatment outcomes between nonsurgical and surgical treatment of distal radius fracture in elderly: a systematic review and meta-analysis. Langenbecks Arch Surg. 2015;400(7):767-779. doi: 10.1007/s00423-015-1324-9
- Campochiaro G, Gazzotti G, Rebuzzi M, Tronci V, Tsatsis C, Catani F. Distal radius articular fractures: a comparison between ORIF with angular stability plate and percutaneous Kirschner wires. Acta Biomed. 2013;84(1):38-43.
- Saving J, Ponzer S, Enocson A, Mellstrand Navarro C. Distal radius fractures—Regional variation in treatment regimens. PLoS One. 2018;13(11):1-11. doi: 10.1371/journal.pone.0207702
- Özkan S, Westenberg RF, Helliwell LA, Mudgal CS. Distal radius fractures: evaluation of closed reduction and percutaneous kirschner wire pinning. J Hand Microsurg. 2018;10(03):134-138. doi: 10.1055/s-0038-1648334
- Achten J, Sones W, Dias J, Hedley H, Cook JA, Dritsaki M, et al. Surgical fixation with K-wires versus plaster casting in the treatment of dorsally displaced distal radius fractures: protocol for distal radius acute fracture fixation trial 2 (DRAFFT 2). BMJ Open. 2019;9(3):1-7. doi: 10.1136/bmjopen-2018-028474
- Costa ML, Achten J, Parsons NR, Rangan A, Griffin D, Tubeuf S, et al. Percutaneous fixation with Kirschner wires versus volar locking plate fixation in adults with dorsally displaced fracture of distal radius: randomised controlled trial. BMJ. 2014;349:1-10. doi: 10.1136/bmj.g4807
- Toon DH, Premchand RA, Sim J, Vaikunthan R. Outcomes and financial implications of intra-articular distal radius fractures: a comparative study of open reduction internal fixation (ORIF) with volar locking plates versus nonoperative management. J Orthop Traumatol. 2017;18(3):229-234. doi: 10.1007/s10195-016-0441-8
- Sengab A, Krijnen P, Schipper IB. Displaced distal radius fractures in children, cast alone vs additional K-wire fixation: a meta-analysis. Eur J Trauma Emerg Surg. 2019;45(6):1003-3011. doi: 10.1007/s00068-018-1011-y
- Franceschi F, Franceschetti E, Paciotti M, Cancilleri F, Maffulli N, Denaro V. Volar locking plates versus K-wire/pin fixation for the treatment of distal radial fractures: a systematic review and quantitative synthesis. Br Med Bull. 2015;115(1):91-110. doi: 10.1093/bmb/ldv015
- Cummings SR, Kelsey JL, Nevitt MC, O’DOWD KJ. Epidemiology of osteoporosis and osteoporotic fractures. Epidemiol Rev. 1985;7(1):178-208. doi: 10.1093/oxfordjournals.epirev.a036281
- Hull P, Baraza N, Gohil M, Whalley H, Mauffrey C, Brewster M, et al. Volar locking plates versus K-wire fixation of dorsally displaced distal radius fractures—a functional outcome study. J Trauma Acute Care Surg. 2011;70(6): E125-E128. doi: 10.1097/TA.0b013e3181e32714
- Rozental TD, Blazar PE, Franko OI, Chacko AT, Earp BE, Day CS. Functional outcomes for unstable distal radial fractures treated with open reduction and internal fixation or closed reduction and percutaneous fixation: a prospective randomized trial. J Bone Joint Surg. 2009;91(8):1837-1846. doi: 10.2106/JBJS.H.01478
- Orbay JL, Touhami A. Current concepts in volar fixed-angle fixation of unstable distal radius fractures. Clin Orthop Relat Res. 2006;445:58-67. doi: 10.1097/01.blo.0000205891.96575.0f
- Costa ML, Achten J, Rangan A, Lamb SE, Parsons NR. Percutaneous fixation with Kirschner wires versus volar locking-plate fixation in adults with dorsally displaced fracture of distal radius: five-year follow-up of a randomized controlled trial. Bone Joint J. 2019;101(8):978-983. doi: 10.1302/0301-620X.101B8.BJJ-2018-1285.R1
- Van Aaken J, Beaulieu JY, Della Santa D, Kibbel O, Fusetti C. High rate of complications associated with extrafocal kirschner wire pinning for distal radius fractures. Chir Main. 2008;27(4):160-166. doi: 10.1016/j.main.2008.05.005
- Yu X, Yu Y, Shao X, Bai Y, Zhou T. Volar locking plate versus external fixation with optional additional K-wire for treatment of AO type C2/C3 fractures: a retrospective comparative study. J Orthop Surg Res. 2019;14(1):1-8. doi: 10.1186/s13018-019-1309-4
- Yetkin H, Altay T, Ozan F, Kayalı C, Koyuncu S. Comparison of open reduction volar locking plate fixation and closed reduction percutaneous K-wire fixation in the treatment of AO type C1 distal radius fractures. Int J Clin Exp Med. 2017;10(1):1139-1144.
- Navarro CM, Ahrengart L, Törnqvist H, Ponzer S. Volar locking plate or external fixation with optional addition of K-wires for dorsally displaced distal radius fractures: a randomized controlled study. J Orthop Trauma. 2016;30(4):217-224. doi: 10.1097/BOT.0000000000000519
- Zink JV, Souteyrand P, Guis S, Chagnaud C, Le Fur Y, Militianu D, et al. Standardized quantitative measurements of wrist cartilage in healthy humans using 3T magnetic resonance imaging. World J Orthop. 2015; 6(8): 641-648. doi: 10.5312/wjo.v6.i8.641
- Wright TW, Horodyski M, Smith DW. Functional outcome of unstable distal radius fractures: ORIF with a volar fixed-angle tine plate versus external fixation. J Hand Surg. 2005;30(2):289-299. doi: 10.1016/j.jhsa.2004.11.014
- Richard MJ, Wartinbee DA, Riboh J, Miller M, Leversedge FJ, Ruch DS. Analysis of the complications of palmar plating versus external fixation for fractures of the distal radius. J Hand Surg. 2011;36(10):1614-1620. doi: 10.1016/j.jhsa.2011.06.030
- Esposito J, Schemitsch EH, Saccone M, Sternheim A, Kuzyk PR. External fixation versus open reduction with plate fixation for distal radius fractures: a meta-analysis of randomised controlled trials. Injury. 2013;44(4):409-416. doi: 10.1016/j.injury.2012.12.003
- Beversdorf DQ, White DM, Chever DC, Hughes JD, Bornstein RA. Central β-adrenergic modulation of cognitive flexibility. Neuroreport. 2002;13(18):2505-2507.
- Egol K, Walsh M, Tejwani N, McLaurin T, Wynn C, Paksima N. Bridging external fixation and supplementary Kirschner-wire fixation versus volar locked plating for unstable fractures of the distal radius: a randomised, prospective trial. J Bone Joint Surg Br. 2008;90(9):1214-1221. doi: 1302/0301-620X.90B9.20521
- Shukla R, Jain RK, Sharma NK, Kumar R. External fixation versus volar locking plate for displaced intra-articular distal radius fractures: a prospective randomized comparative study of the functional outcomes. J Orthop Traumatol. 2014;15(4):265-270. doi: 10.1007/s10195-014-0317-8
- Gouk C, Ng SK, Knight M, Bindra R, Thomas M. Long term outcomes of open reduction internal fixation versus external fixation of distal radius fractures: A meta-analysis. Orthop Rev (Pavia). 2019; 11(3): 1-5. doi: 10.4081/or.2019.7809
- Julfiqar AP, Huda N, Ahmed W. Closed reductions and percutaneus ‘K’wire fixation for adolescent intercondylar fractures of the distal humerus. J Clin Diagn Res. 2013; 7(8): 1666-1668. doi: 10.7860/JCDR/2013/5695.3227
- Orbay JL, Fernandez DL. Volar fixation for dorsally displaced fractures of the distal radius: a preliminary report. J Hand Surg. 2002;27(2):205-215. doi: 10.1053/jhsu.2002.32081
This is an open-access article distributed under the terms of the CreativeCommons Attribution License (CC BY) 4.0 https://creativecommons.org/licenses/by/4.0/