By Maryam Faiz Qureshi1, Ambreen Usmani2, Ayesha Mehwish2, Yasmeen Mahar2, Maria Azam Khattak2, Rida Rubab Ahmed3
AFFLIATIONS:
- Department of Anatomy, Karachi Institute of Medical Sciences, Karachi, Pakistan.
- Department of Anatomy, Bahria University Medical and Dental College, Karachi, Pakistan.
- Department of Anatomy, Bahawalpur Medical and Dental College, Bahawalpur, Pakistan.
DOI: https://doi.org/10.36283/PJMD11-3/007
ORCID iD: 0000-0002-2519-0547
How to cite: Qureshi MF, Usmani A, Mehwish A, Mahar Y, Khattak MA, Ahmed RR. Anatomical Variations of Rhinogenic Headache and Its Relation with Sinusitis: A Computerized Tomography (CT) Scan Study. Pak J Med Dent. 2022;11(3): 37-43. doi: 10.36283/PJMD11-3/007
Background: Variable anatomy, hallmark of sinonasal region is the reason for the etiology of sinonasal symptoms such as rhinogenic headache. This study aimed to investigate the incidence of anatomical variations of the nasal cavity and paranasal sinuses in sinusitis patients with complaint of rhinogenic headache on computed tomography of paranasal sinuses, and the correlation of these variants with a rhinogenic headache.
Methods: A prospective cross-sectional study (n=50) of 18-60 years having sinusitis with rhinogenic headache was steered at the Department of Radiology in the PNS Shifa Hospital of Karachi, Pakistan, between June-December 2021. After obtaining written informed consent, all subjects were investigated for various anatomical variants of the sinonasal region detected on computed tomographic scans of paranasal sinuses and were correlated with a rhinogenic headache. The Chi-square test and Pearson correlation were applied for statistical analysis and the level of significance was set at p≤ 0.05.
Results: The most common anatomical variant of sinonasal region detected was agger nasi cells 32(64%) (Right: r/r -0.24, p =0.09; Left: r/r -0.28, p = 0.04), followed by deviated nasal septum 28(56%) (r/r 0.04, p= 0.75), concha bullosa 23(46%) (r/r 0.07, p=0.59), deviated nasal septum with bony spur (r/r 0.07, p=0.62) and other variants. The overall, study found male (68%) predominance. Significant association existed between rhinogenic headache and some of the anatomical variants along with sinus mucosal thickening (p<0.05).
Conclusion: The significant association (p<0.05) was found between rhinogenic headache and different anatomical variants like agger nasi cells, left-sided agger nasi cells, right-sided Haller’s cells, left-sided maxillary and ethmoid sinusitis.
Keywords: Rhinogenic Headache; CT-PNS; Sinonasal Region; Anatomical Variants.
The term rhinogenic headache (RH) has been an important topic of research for several years and due to its complexity further exploration of the symptom is important. Although, it is a widespread pain syndrome that involves the region around the nasal cavity and orbit in subjects with underlying diseases and deformation its etiology, pathology, association with sinusitis, sinus anatomic variants and treatment are still unclear. The International Headache Society (IHS) has classified recognized RH, despite the limited reported evidence of the existence of RH1. RH is a distinct type of headache that has received an amplified amount of consideration in literature over the past 20 years. Rhinogenic headache is an important symptom for all medical professionals as physicians face difficulty in recognizing the reason behind this distinct type of headache which may be associated with variable anatomy of the sinonasal region. Hence due to its frequency in misdiagnosis, it remains a matter of research and discussion in literature2.
Sinusitis is caused due to anatomical-variations resulting in obstruction or blockage, various other infections, or allergies which affects the quality of human life significantly for more than 5% of the population3. According to Alshaikh and Aldhurais, some of the areas near paranasal sinuses like orbit with relation to the presence of Haller-cells in orbital-floor, anterior-cranial-fossa injury due to aerated crista-galli, optic-nerve trauma due to variable anatomy are at great risk for significant injuries with consequential intra-operative complications. Hence the knowledge of anatomical variations of the sinonasal region is crucial for endoscopic surgeons as well as for radiologists for preoperative assessment and to avoid iatrogenic intra-operative and post-surgical complications. In every case of sinus-mucosal disease whether inflammatory or non-inflammatory the etiopathology of RH is unclear and the cause behind RH being poorly defined is widely debated4.
Nowadays the term rhinogenic headache is used increasingly, but at the same time, it is frequently a misdiagnosis because of difficulty in finding a widely-acceptable description of RH which can lead to unsuitable treatment strategies1. This distinct type of headache should not be overlooked or mixed with other types of aches such as migraine, stress headaches and many other types. Other conditions should be excluded carefully. The proper diagnosis is required to provide quality of patient’s life to reduce suffering from RH due to sinus-mucosal thickening, or various anatomical-factors5-7.
Literature search shows that authors have anticipated a correlation between the presence of RH and sinonasal anatomical variants. In this regard, computed tomography (CT) plays a vital role in identifying various sinus findings including normal anatomy, pathology and anatomical variants such as deviated-nasal-septum (DNS), concha-bullosa (CB) and many other variants that could participate in the etiology of RH8,9. Many anatomical variations of the nasal cavity and paranasal sinuses may be a causative factor for RH. In the literature search, very few studies are done regarding this distinct type of headache and its correlation with anatomical variants detected on CT-PNS. To highlight the importance of this widespread pain syndrome which is often overlooked because of many reasons that could be an ill-defined description of RH, less knowledge of anatomical variants and many others. The present study was designed to observe the prevalence of various anatomical variants of nasal cavity and PNS along with its correlation with RH.
This research was a cross-sectional study (n=50), conducted between June-December 2021, in the Department of Radiology in PNS Shifa Hospital of Karachi. The Institutional Review Board (IRB) of Bahria University Medical and Dental College, approved this research with the ERC reference number: 63/2021. The methodology was elucidated to all subjects and clarification about the procedure of the study was given, if required.
Non-Probability-sampling technique and OpenEpi version 3 calculator was used for sample size. The total duration of the study was 6 months. The symptomatic subjects of sinusitis having RH, which were recruited and diagnosed from ENT-Department to the Radiology-Department, for CT-PNS were considered for this study. The inclusion criteria of this research were subjects symptomatic of sinusitis including both genders ranging from 18-60 years having RH, the radiologically mucosal thickness of sinus more than 1 mm. The exclusion criteria included facial trauma, sinonasal polyposis, malignancy, fungal infection, previous sinus surgery, other types of headaches such as migraine/stress/chronic headaches and pregnant females. All subjects were investigated for various anatomical variations of the sinonasal region including the septum, turbinate, uncinate-process, ethmoidal-cells, sinus-hypoplasia, and asymmetry of sinus cavities. The subjects fulfilling the inclusion conditions and those who were willing to participate obtained written informed consent.
After taking detailed history including demographic data, symptoms, and physical examination, subjects were considered for CT-PNS. The CT scan was done in both view coronal and axial. Toshiba’s 160-slice-Prime Aquilion CT scan was used for radiography. The prone position was considered for the coronal imaging and hard-palate was made as to the point of reference and the plane of section was perpendicular to the hard palate. Direct scans were made from the frontal sinus (anterior wall) and sphenoid sinus (posterior wall). The axial view imaging was done in the supine position and the orbitomeatal-line was considered as the reference point. The slice-thickness was 3 mm thick and the computed tomographic exposure settings were 120 kV and 80 mAs. In the tomography reporting room, the scans were analyzed for all the possible findings including various anatomical variations of the nasal cavity and paranasal sinuses. After complete reporting of every subject, all anatomical variations of the nasal cavity and paranasal sinuses were noted on the proforma.
The research data were analyzed by using Statistical Package for Social Sciences version-23.0 for Windows (SPSS). For quantitative and qualitative variables mean, standard deviation, frequency and percentages were calculated. The Chi-square and Pearson correlation was applied for the statistical analysis. The level of significance was set at p≤ 0.05.
The mean age of study participants was 42.68±18.22. The overall study found male predominance with a reported frequency of 68% and 32% of females having sinusitis associated with RH as shown in Figure 1.
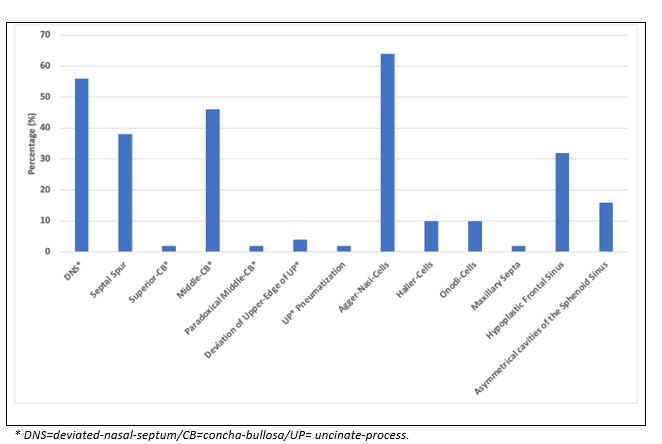
Figure 1: Frequency of anatomical variations of sinonasal region.
The presence of anatomical variations of the nasal cavity and paranasal sinuses was observed in all study participants with variable frequencies (Table 1). A significant association existed between Rhinogenic headache (RH) and agger-nasi-cells with a p-value of 0.04. No other significant association was observed between anatomical-variant of the nasal cavity along with PNS and RH (Table 1).
Table 1: Anatomical variations of nasal cavity and paranasal sinuses (PNS) and its correlation with Rhinogenic Headache (RH).
| Anatomical Variants | No. of Subjects (N=50)
Frequency (%) |
Rhinogenic Headache | |
| r/r | p-Value | ||
| DNS* | 28(56.0) | 0.04 | 0.75 |
| Septal Spur | 19(38.0) | -.01 | 0.94 |
| Superior-CB* | 1(2.0) | -.13 | 0.34 |
| Middle-CB* | 23(46.0) | 0.07 | 0.59 |
| Paradoxical Middle-CB* | 1(2.0) | 0.14 | 0.30 |
| Deviation of Upper-Edge of UP* | 2(4.0) | -.19 | 0.17 |
| UP* Pneumatization | 1(2.0) | -1.37 | 0.34 |
| Agger-Nasi-Cells | 32(64.0) | -.28 | 0.04* |
| Haller-Cells | 5(10.0) | 0.21 | 0.13 |
| Onodi-Cells | 5(10.0) | -.05 | 0.71 |
| Maxillary Septa | 1(2.0) | -.13 | 0.34 |
| Hypoplastic Frontal Sinus | 16(32.0) | -.14 | 0.31 |
| Asymmetrical cavities of the Sphenoid Sinus | 8(16.0) | -.09 | 0.52 |
*DNS=deviated-nasal-septum/CB=concha-bullosa/UP=uncinate-process;
p-value significant = ≤ 0.05/ρ=r=rho=Pearson correlation co-efficient.
A significant association was found between left-sided agger-nasi-cells and RH with a p-value of 0.04, in addition to it, significant association existed between right-sided Haller-cells and RH with a p-value of 0.03. When other variants were correlated with RH non-significant results were observed whereas a significant association was found between left-sided maxillary, ethmoid sinusitis, and RH with a p-value of 0.03, 0.05 respectively while no other significant association was observed between sinus-mucosal thickening and RH (Table 2). A Scatter plot representing overall significant p-values against frequency is shown in Figure 2.
Table 2: Correlation between right and left-sided anatomical variations of the nasal cavity and paranasal sinuses (PNS) along with PNS-sinusitis involvement with Rhinogenic Headache (RH).
| Anatomical variants and Sinus mucosal thickening (Sinusitis) | Rhinogenic Headache | |||
| Right | Left | |||
| r/r | p-Value | r/r | p-Value | |
| Agger-Nasi-cells | -.24 | 0.09 | -.28 | 0.04* |
| Onodi-cells | -.05 | 0.71 | -.05 | 0.71 |
| CB* | 0.11 | 0.43 | -.04 | 0.73 |
| Haller-Cells | 0.30 | 0.03* | 0.21 | 0.13 |
| DNS* | 0.02 | 0.89 | 0.07 | 0.63 |
| DNS* with Spur | 0.07 | 0.62 | -.02 | 0.85 |
| Maxillary | 0.12 | 0.38 | 0.30 | 0.03* |
| Ethmoid | 0.23 | 0.09 | 0.27 | 0.05* |
| Frontal | 0.15 | 0.26 | 0.01 | 0.93 |
| Sphenoid | 0.01 | 0.93 | 0.15 | 0.26 |
*DNS=deviated-nasal-septum/CB=concha-bullosa/UP=uncinate-process;
p-value significant = ≤ 0.05/ρ=r=rho=Pearson correlation co-efficient.
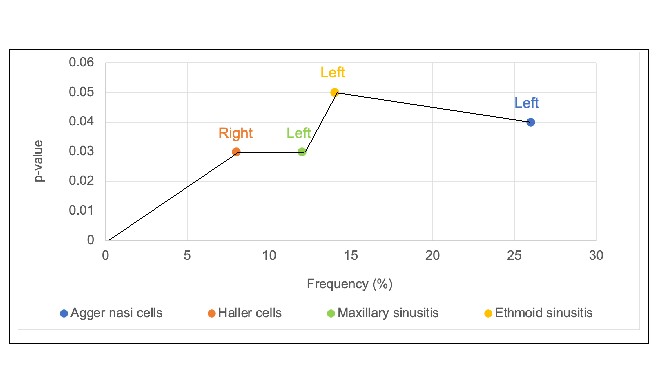
Figure 2: p-value vs frequency of anatomical variants and involved sinus based on significant p-values.
The rhinogenic headache is defined as intermittent pain which is usually referred to in the supraorbital region medially or pain located over the temporozygomatic-region and lasts for four hours, and relapse is observed frequently. In addition to the endoscopic examination, a CT scan of paranasal sinus cavities (CT-PNS) is strictly recommended before planning any proper therapeutic strategy for RH10.
In this study overall males outnumbered females and this finding was supported by Adnan et al., Bakheet and Bakheet and La Mantia et al. concerning gender-based frequency in studies done in the last few years11-13. The results of the current study are witnessing that anatomical variants are the reason for the rhinogenic headache in sinusitis patients. Cantone et al. and Peric et al. believe that anatomical variants like ethmoidal cells, turbinate pneumatization and concha bullosa (CB) are the frequent variants observed in subjects with a rhinogenic headache. And out of these variants, middle turbinate concha-bullosa is strongly associated with the etiology of RH and can be considered as a causative factor for this distinct type of headache and should be considered for surgical treatment strategies10,14,15. The present study contradicts these findings as no significant association was observed between CB and RH.
Among ethmoidal cells, the agger nasi cells were the most prominent variant responsible for the occurrence of rhinogenic headaches in patients with sinusitis. A significant association between ethmoidal cells (agger-nasi-cells, Haller-cells) and RH with significant p-values of 0.04 and 0.03 was observed respectively. One of the studies yielded a statistically significant correlation was observed between frontoethmoidal cells and RH10. This important finding suggests their probable role in dysfunctional ventilation of the frontal sinus, maybe because of their anatomical location close to frontal recess. The occurrence of ethmoidal and frontal cells may become a source of compression, and also adversely affect sinus drainage and ventilation hence resulting in sinus infections and a reason for rhinogenic headache16. This can be correlated with the results of the present study as a significant association was observed between left-sided maxillary sinusitis and ethmoid sinusitis and RH with a p-value of 0.03, and 0.05 respectively. Research shows that very few studies are done related to this topic in which both the sinus-mucosal infection and anatomical variants of the sinonasal region are correlated with RH16-19. Some authors have investigated the prevalence of frontal cells and only a few studies are done in which the association of these cells with RH was observed20-22.
The RH poses a particular diagnostic and therapeutic challenge to various medical personnel. The identification and pathophysiology behind this ache are still not well understood but studies support the strategy of surgical correction of this ache with various endoscopic surgeries23. There has been advancement in the surgical management of sinusitis in recent years, particularly in endoscopic sinus and nasal surgeries, which requires the radiologist to identify the various sinus and nasal anatomical variants, to make aware the surgeon have detailed knowledge of sinonasal-anatomy and anatomical variants, many of these anatomical-variations are detectable only using computed tomography23-25.
To highlight the significance of anatomical variants and their relation with clinical symptoms the present study was conducted to observe the presence of extremely complex anatomical variants of nasal region and PNS in patients suffering from sinusitis associated with RH and correlated these anatomical variants and mucosal thickening of the involved sinuses with RH. The study yielded that mostly male gender was involved in this type of headache associated with sinusitis and at the same time study suggest that anatomical variants were more prevalent in males as compared to females. The results of the present study showed that the significant association between anatomical variants and sinus-mucosal infection with rhinogenic headache gives a clue of their strong association of causing this distinct type of headache. The RH impose critical challenge in both ways’ diagnostic as well as therapeutic. CT-PNS reveals multiple complex anatomical variations of the nasal cavity and paranasal sinuses which may become a reason for RH. It is very important to correlate these anatomic variants with the clinical symptom of sinusitis such as RH.
A significant association existed between rhinogenic headache (RH) and agger-nasi-cells, and between left-sided agger-nasi-cells and right-sided Haller-cells. The left-sided maxillary and ethmoid sinusitis also showed significant results. Though these findings explain a close association between RH and some anatomical variants. Moreover, studies correlating changes in clinical symptoms or RH after surgical treatment of various anatomical variants along with sinus-mucosal contact points are still required.
The authors would like to thank Bahria University Medical and Dental College and PNS Shifa Hospital, Karachi for the facilitation and smooth conduction of the research.
The authors declared no conflict of interest.
The ethical committee/institutional review board (IRB) of Bahria University Medical and Dental College Karachi approved the study with the reference number: 63/2021.
Informed consent was taken from the parents/guardian of the patients.
MFQ did the conceptualization, data curation, and writing. AU supervised the research. AM assisted in the literature search. YM and MAK performed the critical analysis whereas RRA assisted in the data interpretation.
- Barinsky GL, Hanba C, Svider PF. Rhinogenic headache in children and adolescents. Curr Pain Headache Rep. 2020;24(3):1-5. doi: 10.1007/s11916-020-0839-0
- Altin F, Haci C, Alimoglu Y, Yilmaz S. Is septoplasty effective rhinogenic headache in patients with isolated contact point between inferior turbinate and septal spur? Am J Otolaryngol. 2019;40(3):364-367. doi: 10.1016/j.amjoto.2019.02.002
- Mareev OV, Aleshkina OY, Mareev GO, Kuchmin VN, Afonina OI, Kapustina NY. Variability of linear parameters of frontal sinuses in adults. Saratov J Med Sci Res. 2018;14(2):302-305.
- Alshaikh N, Aldhurais A. Anatomic variations of the nose and paranasal sinuses in Saudi population: computed tomography scan analysis. Egypt J Otolaryngol. 2018;34(4):234-241. doi: 10.4103/1012-5574.244904
- Kirsch CF. Headache caused by sinus disease. Neuroimaging Clin. 2019;29(2):227-241. doi: 10.1016/j.nic.2019.01.003
- Herzallah IR, Hamed MA, Salem SM, Suurna MV. Mucosal contact points and paranasal sinus pneumatization: does radiology predict headache causality? Laryngoscope. 2015;125(9):2021-2026. doi: 10.1002/lary.25194
- Jayawardena AD, Chandra R. Headaches and facial pain in rhinology. Am J Rhinol Allergy. 2018;32(1):12-15. doi: 10.2500/ajra.2018.32.4501
- Yeo NK, Park WJ, Ryu IS, Lim HW, Song YJ. Is facial or head pain related to the location of lesions on computed tomography in chronic rhinosinusitis? Ann Otol Rhinol Laryngol. 2017;126(8):589-596. doi: 10.1177/0003489417717268
- Qureshi MF, Usmani A. A CT-Scan review of anatomical variants of sinonasal region and its correlation with symptoms of sinusitis (nasal obstruction, facial pain and rhinorrhea). Pak J Med Sci. 2021; 37(1): 195-200. doi: 10.12669/pjms.37.1.3260
- Sollini G, Mazzola F, Iandelli A, Carobbio A, Barbieri A, Mora R, et al. Sino-nasal anatomical variations in rhinogenic headache pathogenesis. J Craniofac Surg. 2019;30(5):1503-1505. doi: 10.1097/SCS.0000000000005239
- Adnan A, Khan S, Javaid M, Shahabi I, Haq A. Rhinogenic headache and its management. J Med Sci. 2015;23(4):206-208.
- Bakheet E, Bakheet T. Prevalence of anatomical abnormalities of nose and paranasal sinuses in cases of rhinogenic headache among Sohag University students. Sohag Med J. 2020;24(1):140-149. doi: 10.21608/smj.2019.16715.1056
- La Mantia I, Grillo C, Andaloro C. Rhinogenic contact point headache: surgical treatment versus medical treatment. J Craniofac Surg. 2018;29(3):228-230. doi: 10.1097/SCS.0000000000004211
- Cantone E, Castagna G, Ferranti I, Cimmino M, Sicignano S, Rega F, et al. Concha bullosa related headache disability. Eur Rev Med Pharmacol Sci. 2015;19(13):2327-2330.
- Peric A, Rasic D, Grgurevic U. Surgical treatment of rhinogenic contact point headache: an experience from a tertiary care hospital. Int Arch Otorhinolaryngol. 2016;20:166-171. doi: 10.1055/s-0036-1578808
- Tran LV, Ngo NH, Psaltis AJ. A radiological study assessing the prevalence of frontal recess cells and the most common frontal sinus drainage pathways. Am J Rhinol Allergy. 2019;33(3):323-330. doi: 10.1177/1945892419826228
- Okuni T, Takano K, Nomura K, Yamashita K, Abe A, Ito F, et al. Radiological assessment of the anatomy of frontal recess cells and the anterior ethmoidal artery. Excell Otolaryngol. 2016;77: 46-51.
- Johari HH, Mohamad I, Sachlin IS, Aziz ME, Mey TY, Ramli RR. A computed tomographic analysis of frontal recess cells in association with the development of frontal sinusitis. Auris Nasus Larynx. 2018;45(6):1183-1190. doi: 10.1016/j.anl.2018.04.010
- Choby G, Thamboo A, Won TB, Kim J, Shih LC, Hwang PH. Computed tomography analysis of frontal cell prevalence according to the International Frontal Sinus Anatomy classification. Int Forum Allergy Rhinol. 2018;8(7): 825-830. doi: 10.1002/alr.22105
- Marzetti A, Mazzone S, Tedaldi M, Topazio D, Passali FM. The role of balloon sinuplasty in the treatment of vacuum rhinogenic headache. Indian J Otolaryngol Head Neck Surg. 2017;69(2):216-220. doi: 10.1007/s12070-017-1086-5
- Folbe AJ, Svider PF, Eloy JA. Anatomic considerations in frontal sinus surgery. Otolaryngol Clin North Am. 2016;49(4):935-943. doi: 10.1016/j.otc.2016.03.017
- Farmer RL, Garg RK, Afifi AM, Hochman M. Rhinogenic Headaches. In Surgical Treatment of Chronic Headaches and Migraines 2020 (pp. 103-117). Springer, Cham. doi: 10.1007/978-3-030-36794-7_9
- Lingaiah RK, Puttaraj NC, Chikkaswamy HA, Nagarajaiah PK, Purushothama S, Prakash V, et al. Anatomical variations of paranasal sinuses on coronal CT-scan in subjects with complaints pertaining to PNS. Radiol Sec. 2016;20169:1-7.
- Swain L, Singh M, Routray PN. Retrospective analysis of anatomical variations of paranasal sinuses on multidetector computed tomography–A randomized cross-sectional study. Ann Int Med Den Res. 2018; 4:15-21.
- Baig S, Asma NK, Patil N. Anatomical variation between columella and sphenoidal sinuses: a study conducted on adult cadavers. Pak J Med Dent. 2017;6(2): 8-12.
This is an open-access article distributed under the terms of the CreativeCommons Attribution License (CC BY) 4.0 https://creativecommons.org/licenses/by/4.0/