By Khaled Abdullah Rage, Maria Ahmed, Amara Zafar, Sana Shahid, Summaya Saeed
AFFLIATIONS:
- Dr. Ruth K.M. Pfau Civil Hospital Karachi, Pakistan.
Traumatic abdominal wall hernia (TAWH) has a reported incidence of around 1%. It is defined as herniation of intra-abdominal organs following trauma without skin penetration. High-energy trauma is often associated with intra-abdominal injury. Treatment options vary from non-operative management to surgical repair either open or laparoscopic. We present a case of a middle-aged male who presented with a history of rickshaw roll over injury. On examination, there was tender abdominal swelling with abrasions. Computerized Tomography (CT) scan confirmed the diagnosis of TAWH and free fluid in abdomen. Emergency exploratory laparotomy was performed. Mesenteric tears were repaired and primary restoration of abdominal wall was done. The patient was discharged on a fourth post-operative day without any complications. Management of TAWH should be tailored according to individual patient presentation. Midline exploratory laparotomy with the primary hernial repair is an operative intervention of choice for those with high-energy injury as there is an increased chance of accompanying visceral trauma.
Keywords: Laparotomy; Trauma; Hernia.
Blunt trauma leading to abdominal wall hernia is a rare condition with reported incidence of around 1% in all patients with abdominal trauma1. First case report on traumatic abdominal wall hernia (TAWH) was published in 1906 2. TAWH is defined as blunt trauma leading to the disruption of anterior abdominal wall musculature and fascia, resulting in herniation of intra-abdominal viscera without skin penetration with no previous history of hernia2. Though blunt abdominal trauma is quite common however, TAWH is quite rare occurrence.
We here present a rare case of TAWH in a patient with a history of rollover injury by rickshaw and associated with intra-abdominal mesenteric tear. The patient was managed surgically in an emergency with an excellent post-operative course.
A 50 years old male patient, resident of Karachi, known case of hypertension and chronic obstructive pulmonary disease (COPD), presented at the accident and emergency department of Dr. Ruth K.M. Hospital Karachi, with the history of road traffic accident. He had a rickshaw rollover injury and suffered a high velocity trauma. His chief complaints at presentation in the emergency department were abdominal pain and swelling which developed immediately after trauma. On presentation, he had a pulse of 110 beats per minute and respiratory rate of around 16 breaths per minute. His blood pressure was 100/60 and he was afebrile. Vitals at the time of presentation in Emergency Department: Pulse 110/minute, Respiratory Rate 16 breaths/minute, Blood Pressure100/60 and Temperature 36.5˚C.
On examination, he was conscious, oriented, and in severe pain. There were no signs of head, chest, pelvic, or limb injury. Primary survey revealed abrasions over anterior abdominal wall. There was a palpable, reducible, and tender abdominal swelling of about 15×10 cm in size. Apart from tachypnoea, his respiratory examination was average. On cardiovascular examination, he had tachycardia; rest of the examination was unremarkable. His motor examination revealed normal tone, bulk, power, and reflexes in all four limbs and a Glasgow Coma Scale (GCS) of 15/15. Rest of the history and general physical examination was typical. According to advanced trauma life support (ATLS) principles his resuscitation was done.
Chest X-ray was done which was unremarkable. Extended focused assessment with sonography for trauma (eFAST) was done which was positive with free fluid in pelvis, perisplenic area, and Morrison’s pouch. Computerized Tomography (CT) scan (Figure 1) was done which showed defect in the anterior abdominal wall with herniated bowel loop and free fluid around liver and spleen. Plan for exploratory laparotomy was made and patient was shifted to emergency operation theatre as there was a history of high velocity trauma. Routine blood investigations were within normal limits.
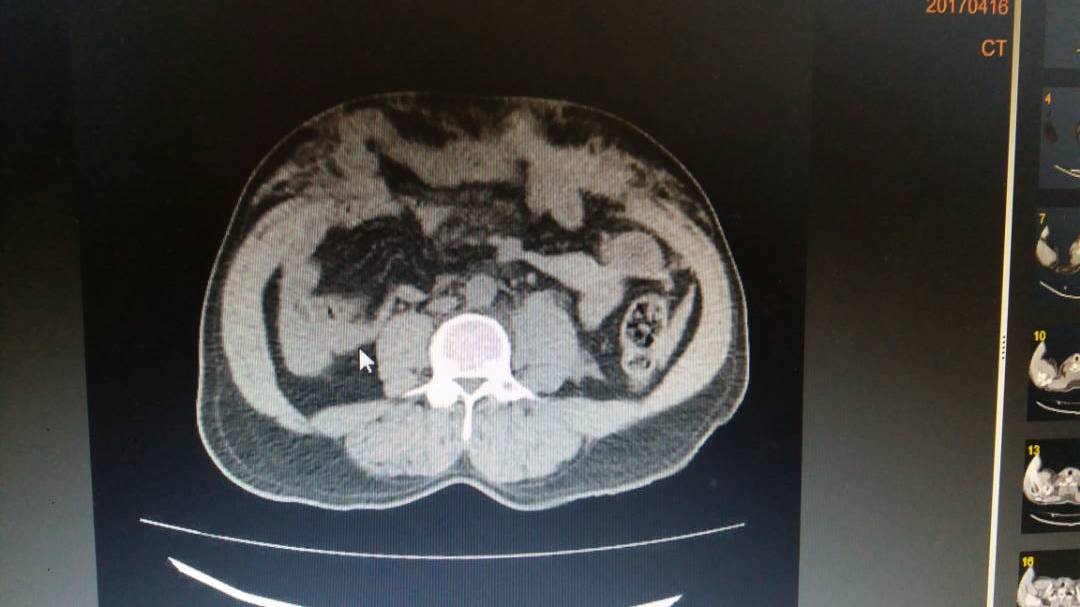
Figure 1: Computed tomography (CT) scan of abdomen showing Traumatic abdominal Wall Hernia (TAWH) indicted by arrow.
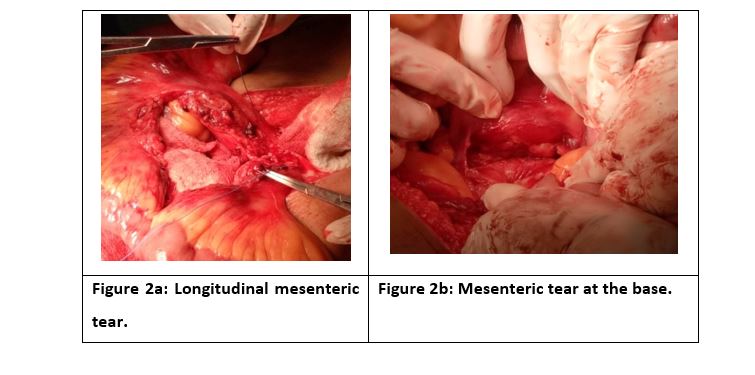
A midline laparotomy incision was given. Perioperative findings included 12cm laceration of anterior abdominal wall muscles with herniated small bowel loops and subcutaneous hematoma, intra-peritoneal clots, 8cm longitudinal mesenteric tear (Figure 2a), 5cm tear at base of mesentery just anterior to its attachment to retroperitoneum (Figure 2b) and serosal tear in the sigmoid colon. No hollow viscus or solid organ injury was found.
Anatomical repair of fascial defect with non-absorbable suture was done and mesenteric tears were repaired with 2/0 vicryl suture. The drain was placed in pelvis and redivac drain was placed in subcutaneous space. On the first post-operative day patient was allowed orally and encouraged to mobilize. His redivac drain output was 45ml while pelvic drain output was 50ml on the first day. Drains were removed on third post-operative day. On fourth post-operative day patient did not have any complication and was discharged and called for a follow up. Four weeks after discharge on the follow up visit the patient was doing well. On his follow up visit after three months, examination showed a healthy healed scar with no palpable defect on clinical examination.
Traumatic abdominal wall hernia (TAWH) is a herniation of intra-abdominal organs after blunt trauma to abdomen leading to the disruption of fascia and musculature of abdominal wall without any skin breach and with no prior history of hernia2. The mechanism of TAWH is thought to be an abrupt surge in intra-abdominal pressure in the presence of high velocity shearing forces that causes the disruption of abdominal wall musculature and fascia leading to subcutaneous herniation of viscera through the defect3. Considering the elasticity of the skin as compared to underlying structures, it remains intact.
The typical location of TAWH is right lower abdomen, lateral to the rectus sheath through oblique and transverse abdominal musculature close to iliac region. As suggested by Yan et al., a high tension of these muscular elements between pelvic bones is responsible for this location of TAWH4. Dennis et al. in their study graded abdominal wall injury with grade one simply being abdominal walls bruises while grade six being complete abdominal wall disruption with evisceration5. In our case, the injury was grade five, which was complete abdominal wall muscle disruption with herniation of abdominal content.
Diagnosis of TAWH is often confirmed with a CT scan to identify the defect, contents of hernia and associated injury. Ultrasonography is considered inferior to CT scans due to its operator dependency and is less sensitive in detecting associated injury. Sometimes the TAWH is confused with subcutaneous hematoma but CT scan helps in differentiating between the two. CT is less reliable in identifying the associated hollow viscus injury or mesenteric tear. The incidence of diaphragmatic herniation is much more as compared to TAWH; however, both can coexist after blunt trauma6,7. A high index of suspicion is required to suspect other intra-abdominal injury. As in our case, the patient was having an associated large mesenteric tear, which was repaired per-operatively.
We are reporting a case of a middle-aged man who presented with TAWH after a rickshaw roll over injury. We observed another case in which a 36-year-old male on a motorcycle who was hit in a road traffic accident was presented with intra-abdominal injuries. Focused assessment with sonography for trauma (FAST) scan was negative for any fluid in his abdomen or pelvis. His CT scan of the abdomen however showed large right lateral abdominal wall disruption involving muscles and fascia with small bowel and colon seen to be herniated via the sonography defection2.
Our patient was immediately shifted to emergency to operation theatre for an exploratory laparotomy based on his history of high velocity trauma which resulted in a quick recovery and a very favourable prognosis. In literature, we see cases where early evaluation with CT scan and emergency, surgery patients had excellent recovery7,8.
A similar case of TAWH was seen in a 25-year-old obese male who was a victim of high-speed road traffic accident. His CT scan of the abdomen showed herniation of the right colon with extensive muscular disruption of the abdominal wall. He was called for a surgical repair of the hernia in 4-6 weeks however he showed up 8 months later with a larger muscular defect resulting in a very large hernia containing both small and large bowel loops1. A delay in timely surgical intervention resulted in a larger hernial defect. However, the appropriate time of surgical intervention varies on a case-by-case basis.
We see a case in literature where a 71-year-old Chinese was operated for a TAWH one year after a car collision where the seat belt had caused a blunt trauma to her lower abdomen. The patient had an emergency laparotomy after the collision but only the ruptures in the ileum were repaired and her hernia was not managed further. She was operated on a year later when she presented with swelling in right lower abdominal quadrant. She was operated without any complication and was doing well after six months follow up9. More recently, we see another case in literature where a 32-year-old-man presented to an emergency department after a fall from height onto a blunt object. The patient presented with abdominal pain and swelling in left flank. CT scan was done which revealed TAWH. Open mesh repair was done and the patient was sent home after third post-operative day10.
Regarding operative management of TAWH, Netto et al. in their retrospective study concluded that first the mechanism of injury should be considered while considering laparotomy and hernial repair as a treatment option. Clinically palpable TAWH is often associated with intra-abdominal injury and needs surgical management immediately. Lastly, the occult hernia does not require urgent laparotomy11. Hence, the management of each case of TAWH needs to be individualized.
Those with high velocity injury often have associated intra-abdominal organ injury and midline exploratory laparotomy with hernia repair should be contemplated. Laparoscopy is suitable in those patients who are vitally stable and having indeterminate CT scan findings. It helps in preventing negative laparotomy and in accurate positioning of dermal incision over TAWH for repair, thus one can avoid large midline laparotomy scar12. TAWH is usually found through a physical exam with pain on palpation and a visible bulge of the abdomen. CT scan is very sensitive in detecting a TAWH. In the remaining cases, TAWH is detected on an exploratory laparotomy.
Although abdominal trauma is a common surgical emergency but traumatic abdominal wall hernia (TAWH) is rare entity associated with it. It can result from both low and high velocity abdominal trauma. CT scan helps in the diagnosis but cannot detect associated intra-abdominal injury. Exploratory laparotomy with primary hernial repair is the best management for those with high velocity injury as there is an increased chance of accompanying visceral trauma.
The authors would like to acknowledge the supervisor for providing the opportunity to report the case.
The authors declare no conflict of interest.
The patient had been informed regarding the study and written consent was taken.
All authors contributed equally to this case study.
- Al Beteddini OS, Abdulla S, Omari O. Traumatic abdominal wall hernia: a case report and literature review. Int J Surg Case Rep. 2016;24:57-59.
- Hamidian Jahromi A, Skweres J, Sangster G, Johnson L, Samra N. What we know about management of traumatic abdominal wall hernia: review of the literature and case report. Int Surg. 2015;100(2):233-239.
- den Hartog D, Tuinebreijer WE, Oprel PP, Patka P. Acute traumatic abdominal wall hernia. Hernia. 2011;15(4):443-445.
- Yan J, Wood J, Bevan C, Cheng W, Wilson G. Traumatic abdominal wall hernia—a case report and literature review. J Pediatr Surg. 2011;46(8):1642-1645.
- Dennis RW, Marshall A, Deshmukh H, Bender JS, Kulvatunyou N, Lees JS, et al. Abdominal wall injuries occurring after blunt trauma: incidence and grading system. Am J Surg. 2009;197(3):413-417.
- Ahmed S, Towbin RB, Towbin AJ. Traumatic abdominal wall hernia. Appl Radiol. 2015; 44(5):1-2.
- Gandhi CS, Kadam P, Mote D, Ingle G. Traumatic abdominal wall hernia: a rare case report and review. Int Surg J. 2016;3(4):2307-2309.
- Singal R, Dalal U, Dalal AK, Attri AK, Gupta R, Gupta A, et al. Traumatic anterior abdominal wall hernia: A report of three rare cases. J Emerg Trauma Shock. 2011; 4(1): 142-145.
- Lyu YX, Ma HY. Case report of traumatic abdominal wall hernia caused by seat belt. Medicine (Baltimore). 2018;97(50):1-4.
- Sharma D, Shrestha S, Ghimire R. Blunt abdominal trauma leading to acute abdominal wall hernia: a case report. Nepal J Med Sci. 2020;5(1):86-90.
- Netto FA, Hamilton P, Rizoli SB, Nascimento Jr B, Brenneman FD, Tien H, et al. Traumatic abdominal wall hernia: epidemiology and clinical implications. J Trauma Acute Care Surg. 2006;61(5):1058-1061.
- Tiong H, So J, Cheah W. Traumatic abdominal wall hernia: open and laparoscopic approaches to repair. Internet J Surg. 2006;10(2):1-4.
This is an open-access article distributed under the terms of the CreativeCommons Attribution License (CC BY) 4.0 https://creativecommons.org/licenses/by/4.0/