By Misauq Mazcuri1, Tanveer Ahmed1, Muhammad Shoaib Lodro1, Ambreen Abid1, Nazish Sikander1, Nadir Ali1
- Thoracic Surgery Department, JPMC, Karachi, Pakistan
DOI: https://doi.org/10.36283/PJMD12-4/016
How to cite: Mazcuri M, Ahmed T, Lodro MS, Abid A, Sikander N, Ali N. Late Presentation of Primary Choriocarcinoma Lung in a Young Male. Pak J Med Dent. 2023;12(4): 86-89. doi: 10.36283/PJMD12-4/016
Primary Choriocarcinoma of the lung is a rare malignant tumor in young patients. It is mostly misdiagnosed as primary or metastatic lung cancer. Poor outcome is seen due to delays in treatment and aggressive behavior of the tumor. We present an 18-year-old male the complaints of chest pain, backache, and hemoptysis. He denied any history of tuberculosis or malignancy though he confirmed to be an occasional smoker. He was tachypneic with decreased air entry bilaterally and the rest of the examination was normal. Investigations revealed multiple bilateral pulmonary nodules. Intraoperatively multiple brown sub-centimeters to more than one-centimeter lung nodules were observed. Histopathology was suggestive of Choriocarcinoma of the lung. Beta-HCG was positive with workup for distant metastasis suggestive of para-aortic lymph node invading left psoas muscle. He was referred to oncology where he expired due to widespread disease and chemotherapy side effects.
Keywords: Choriocarcinoma, Lung Nodules, Germ Cell Tumor, Non-Seminomatous Germ Cell Tumor.
Primary Choriocarcinoma (PCC) is classified into non-gestational and gestational cancer. Most commonly it arises in the genitals followed by the mediastinum and retroperitoneal space. PCC commonly metastasizes to the lung and rarely presents as primary lung pathology 1. They may present with symptoms like hemoptysis, shortness of breath, and chest pain. Radiographic signs of PCC lung are often misinterpreted as metastatic or primary lung cancer, with delayed therapy and a dismal outcome 2, 3. We present a rare case of an 18-year-old male who presented with bilateral multiple lung nodules secondary to PCC.
CASE PRESENTATION
An 18 years old young male patient, an occasional smoker, presented with severe backache, chest pain, shortness of breath, and hemoptysis over the past 15 days. The patient had no family history of malignancy or tuberculosis. At admission, he appeared anxious, with a pulse of 100 beats per minute, blood pressure of 110/70 mmHg, saturation of 92% on room air, and a respiratory rate of 26 breaths per minute. On chest examination, there was decreased bilateral air entry with unremarkable abdominal and scrotal examination.
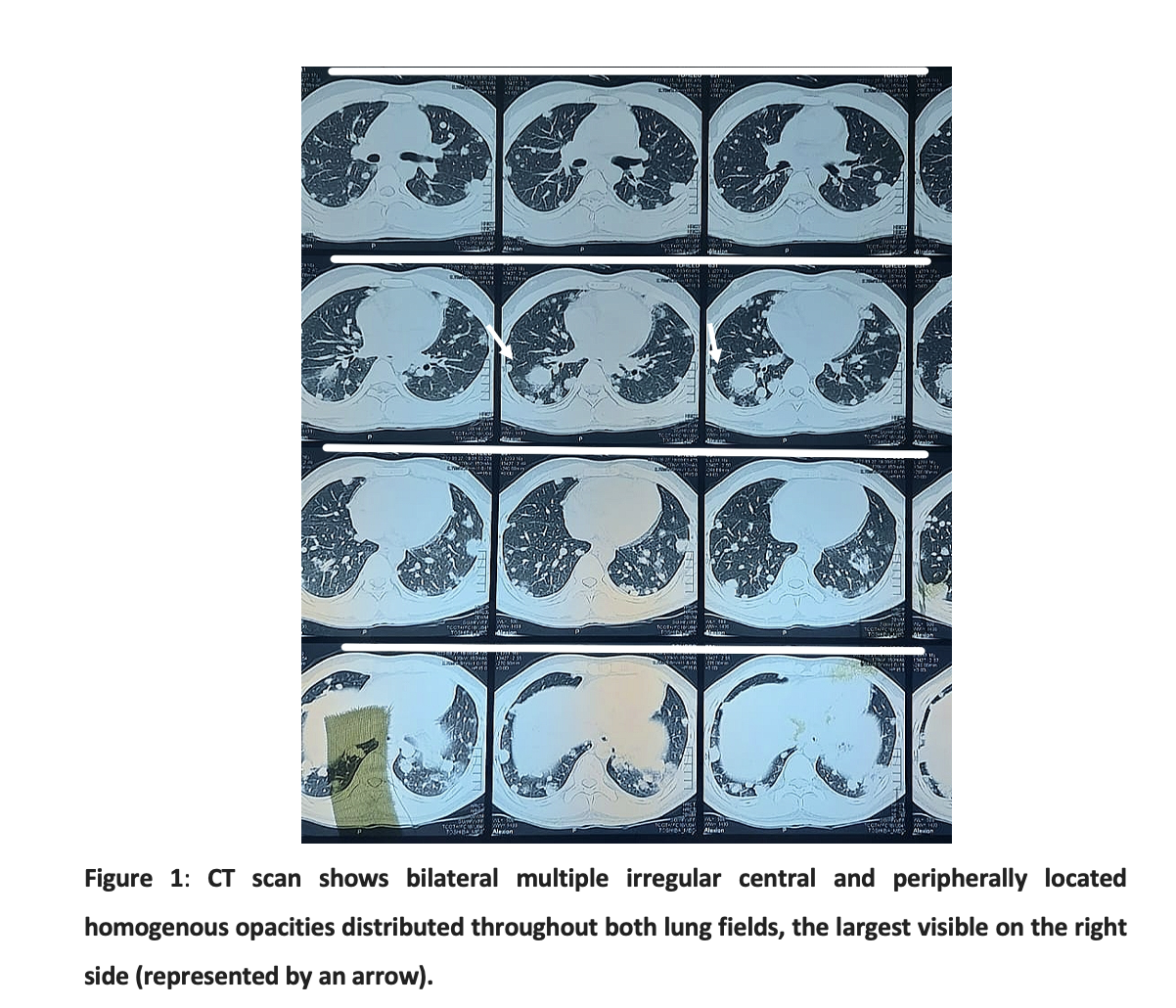
Chest x-ray (CXR) showed bilateral (BL) multiple nodules throughout the lung fields, there was no pleural effusion. Chest tomography (CT) scan demonstrated multiple nodules of variable sizes within both lung fields, the largest one measuring 2.6 x 2.5cm. No lymphadenopathy was noted in the mediastinum. (Figure 1)
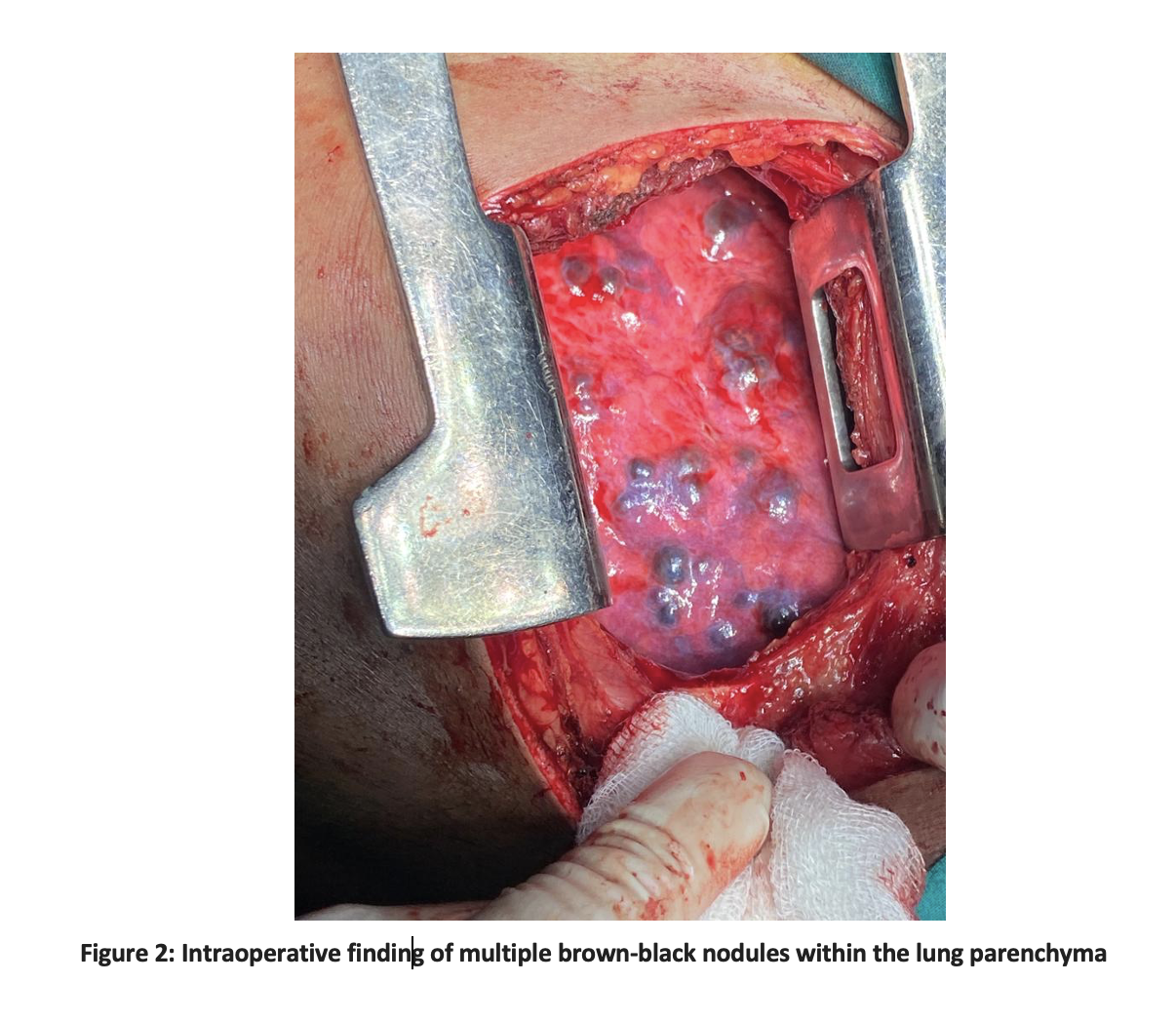
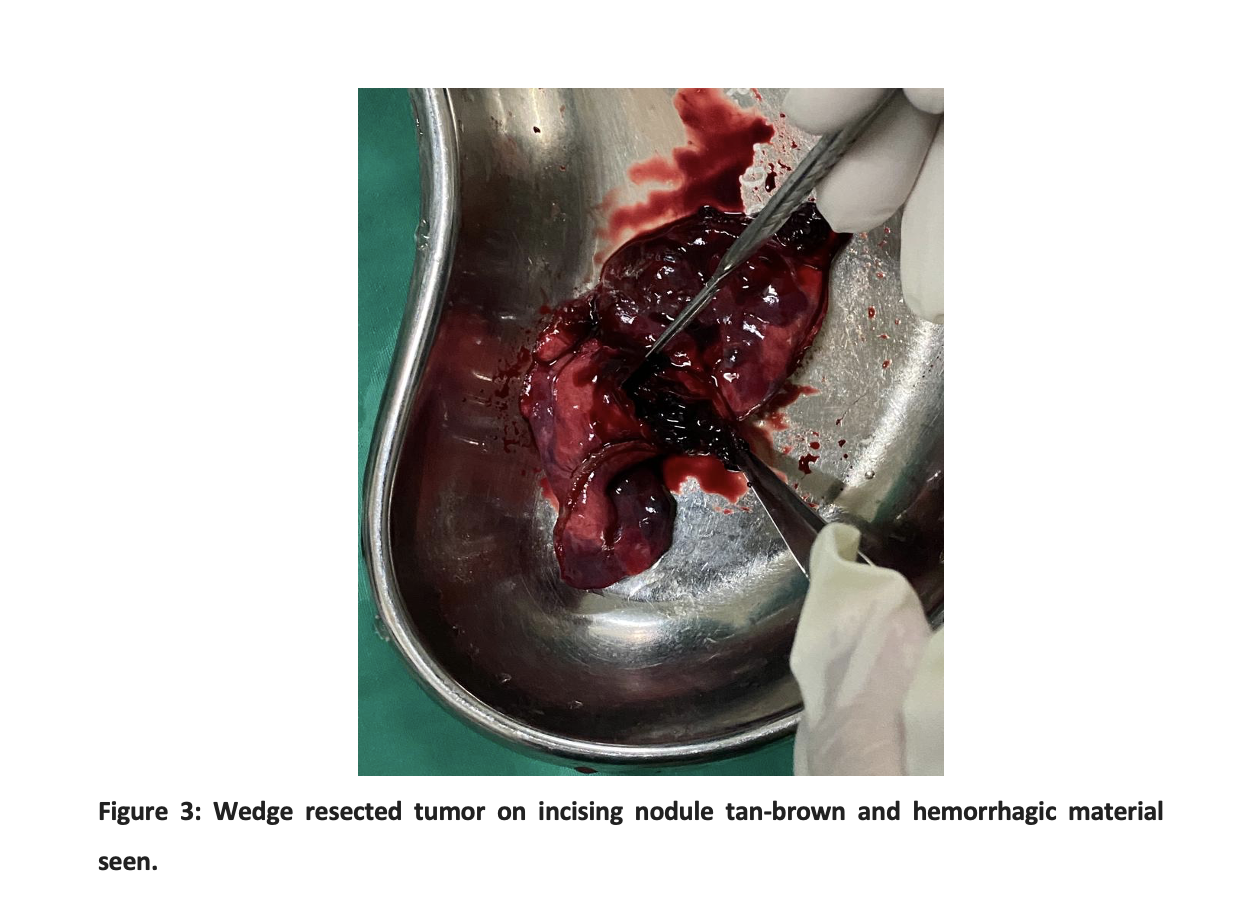
Diagnosis of the malignant metastatic tumor could not be ruled, therefore a wedge biopsy of the left lower lobe of the lung was done. During surgery, multiple brown-black sub-centimeter to more than one-centimeter lung nodules were observed (Figure 2). Grossly cut surfaces were tan-brown and hemorrhagic (Figure 3).
Microscopic examination revealed lung tissue with neoplastic lesions and extensive areas of hemorrhage. The neoplastic lesion was composed of intermediate trophoblastic and multinucleated syncytiotrophoblasts with scattered cytotrophoblasts. Histopathology confirmed the diagnosis of choriocarcinoma with positive immunohistochemistry for Beta HCG. Further Doppler ultrasound scrotum showed normal testes, and a serum Beta HcG level of 2800 u/ml was recorded. CT scan abdomen and pelvis showed retroperitoneal metastatic with Para-aortic lymph nodes invading the left psoas muscle. The diagnosis of primary Choriocarcinoma of the lung with metastasis to the para-aortic lymph nodes was made. The patient was referred to the Oncology department for chemotherapy where Cisplatin-based chemotherapy was started but the patient expired due to respiratory failure secondary to extensive disease progression of the lungs and chemotherapy side effects.
The extra-gonadal germ cell tumors (EGCT) are divided into benign and malignant (EGCT). Malignant EGCT is further divided into seminal germinal tumors (SGCT) and non-seminomatous germinal tumors (NSGCT) 1, 4. PCC is a subtype of NSGCT that can affect both males and females and represents 3% of all germ cell tumors in men, in literature Only 67 cases of PCC in lungs have been identified but only seven cases of PCC with bilateral lung nodules are reported including the current case 5. The main hypothesis for the pathogenesis of PCC in the lung is that the tumor originates from primordial germ cells that abnormally migrate during embryogenesis and continue through adulthood. The other hypothesis suggested that the tumor metastasizes from a primary gonadal choriocarcinoma or that the tumor directly arises in non-gonadal tissues through trophoblastic differentiation 5,6.
Many patients with pulmonary or metastatic PCC may present with symptoms like hemoptysis due to its propensity to grow and invade local vessels. A wide variety of lung lesions can lead to hemoptysis, and therefore the diagnosis of the underlying cause can be difficult 7. In young male patients presenting with normal physical examination and nodules on CXR, tumor markers along with a CT scan from the chest up to the pelvis should be obtained to rule out the primary cause. Beta HCG (b-HCG) level higher than 1000miu/ml is diagnostic of choriocarcinoma therefore treatment should be started without awaiting histologic diagnosis 8. Our case supports this as our patient had a b-HCG level of 2800 µ/ml which indicates the importance of b-HCG as an initial workup before the biopsy.
Management includes surgery, chemotherapy, chemoradiotherapy, or combination therapy 9. Various authors support different management plans, Serno J et al suggested that once the diagnosis is confirmed cisplatin-based chemotherapy without radiotherapy is most commonly used with better outcomes in early disease 10. However, Snoj et al reported improved outcomes in those treated with both surgery and chemotherapy 11. The PCC may metastasize to the lungs, retroperitoneal lymph nodes, bones, and liver. Once the disease metastasizes to other structures, the response may be poorer 10, 12.
Patients presenting with PCC have a median survival of less than one year 9. Factors that have poorer outcomes include tumor size ≥ 5cm, smokers, advanced disease, and those beyond the fourth decade of life 9. Among the cases reported to date, 20% of patients failed to receive any treatment likely secondary to advanced disease 9. In our case, the patient presented with advanced disease where chemotherapy was ineffective and the patient expired within one month of diagnosis due to respiratory failure. We believe that his siblings should be scrutinized for the tumor.
Primary Choriocarcinoma of the lung in an 18-year-old male indicated that low cost and early availability of serum beta HCG level may prevent late diagnosis of PCC. Early chemotherapy improves outcomes with bilateral or unilateral multiple lung nodules in male patients with normal physical examination and ultrasound scrotum. Biopsy via open thoracotomy or thoracoscopy may provide sufficient tissue for histologic and cytological diagnosis in a patient with a small-sized bilateral lung nodule. However, at the same time, it may delay the diagnosis and treatment.
The authors would like to acknowledge the hospital staff for their immense contribution.
The authors declare no conflict of interest.
Informed and written consent was acquired from the patient before the initiation of the write-up of the case report.
All authors equally contributed to the study.
- Snoj Z, Kocijancic I, Skof E. Primary pulmonary choriocarcinoma. Radiol Oncol. 2016 24;51(1):1-7. doi: 10.1515/raon-2016-0038.
- Kim JH, Cha MJ, Kim MK, Chung YJ, Lee EJ. Disseminated Primary Pulmonary Choriocarcinoma Successfully Treated by Chemotherapy: A Case Report and Literature Review. Cancer Invest. 2020;38(8-9):493-501. doi: 10.1080/07357907.2020.1804575.
- .Zhang S, Gao H, Wang XA, Liang B, Li DW, Shao Y, Jiang SJ. Primary choriocarcinoma in mediastinum with multiple lung metastases in a male patient: A case report and a review of the literature. Thorac Cancer. 2014;5(5):463-467. doi: 10.1111/1759-7714.12120.
- Duarte C, Gilbert DM, Sheridan AD, La Rosa FG, McCarter M, Cost NG, Emmons S, Lam ET. Spontaneous regression of an extragonadal seminomatous germ cell tumor. Cancer Treat Res Commun. 2021; 28:100383. doi: 10.1016/j.ctarc.2021.100383.
- Jiang F, Xiang Y, Feng FZ, Ren T, Cui ZM, Wan XR. Clinical analysis of 13 males with primary choriocarcinoma and review of the literature. Onco Targets Ther. 2014; 7: 1135-1141. doi: 10.2147/OTT.S62561.
- Kim JH, Cha MJ, Kim MK, Chung YJ, Lee EJ. Disseminated Primary Pulmonary Choriocarcinoma Successfully Treated by Chemotherapy: A Case Report and Literature Review. Cancer Invest. 2020;38(8-9):493-501. doi: 10.1080/07357907.2020.1804575.
- Shintaku M, Hwang MH, Amitani R. Primary choriocarcinoma of the lung manifesting as diffuse alveolar hemorrhage. Arch Pathol Lab Med. 2006;130(4):540-543. doi: 10.5858/2006-130-540-PCOTLM.
- Shinoda J, Sakai N, Yano H, Hattori T, Ohkuma A, Sakaguchi H. Prognostic factors and therapeutic problems of primary intracranial choriocarcinoma/germ-cell tumors with high levels of HCG. J Neurooncol. 2004;66(1-2):225-240. doi: 10.1023/b:neon.0000013499.74404.81.
- Johnson AM, Johnson CM, Khalil Z, Stitzel M, Teoh D. Case Report: Treatment of primary pulmonary choriocarcinoma with lung lobectomy and adjuvant chemotherapy. Gynecol Oncol Rep. 2022; 43:101064. doi: 10.1016/j.gore.2022.101064.
- Serno J, Zeppernick F, Jäkel J, Schrading S, Maass N, Meinhold-Heerlein I, Bauerschlag DO. Primary pulmonary choriocarcinoma: case report and review of the literature. Gynecol Obstet Invest. 2012;74(2):171-176. doi: 10.1159/000336784.
- Snoj Z., Kocijancic I., Skof E. Primary pulmonary choriocarcinoma. Radiol. Oncol. Mar. 2017;51(1):1
- Rali P, Xie J, Rali G, Rali M, Silverman J, Malik K. A Rare Case of Metastatic Choriocarcinoma of Lung Origin. Case Rep Pulmonol. 2017; 2017:4649813. doi: 10.1155/2017/4649813.
This is an open-access article distributed under the terms of the CreativeCommons Attribution License (CC BY) 4.0 https://creativecommons.org/licenses/by/4.0/