By Zubaida Masood 1, Rahila Imtiaz1, Fauzia Ali 1, Samia Husain 2, Mataa-E-Masood 3, Jarry Masood 4
- Obstetrics and Gynecology Department, Karachi Medical and Dental College, Karachi, Pakistan
- Obstetrics and Gynecology Department, Aziz Medical Center, Karachi, Pakistan
- Jinnah Postgraduate Medical Center, Karachi, Pakistan
- Dow International Medical College, Karachi, Pakistan
DOI: https://doi.org/10.36283/PJMD12-4/010
How to cite: Masood Z, Imtiaz R, Ali F, Husain S, Masood M, Masood J. Challenges Arising from Self-Administered Misoprostol for Unintended Pregnancies Amidst Covid-19 Lockdown. Pak J Med Dent. 2023;12(4): 51-56. Doi: 10.36283/PJMD12-4/010
Background: The COVID-19 pandemic placed unprecedented strain on healthcare globally, which exacerbated factors leading to unplanned pregnancies. This study aimed to assess the complications of self-administration of misoprostol for miscarriage during the COVID-19 lockdown.
Methods: This was a retrospective cohort study conducted at the Department of Obstetrics and Gynecology, Abbasi Shaheed Hospital, Karachi, from 1st March to 30th September 2020. Case records were compiled and analyzed. All women who reported after self-administration of misoprostol were included. The primary outcome measure was complications; anemia, blood transfusion, heavy bleeding, shock, sepsis, ruptured ectopic pregnancy, and ruptured uterus. A bivariable analysis was done to see the effect of gestational age at intake of misoprostol on the complications encountered, the chi-square test or Fischer’s exact test was also applied.
Results: In this study, a total of 54 cases were studied. The most common complication was anemia (63%) followed by incomplete abortion (61.1%). Heavy bleeding (p˂0.001), blood transfusion (p=0.020), and incomplete abortion were significantly (p˂0.001) more common in women who used misoprostol at gestational ages greater than 6 weeks.
Conclusion: Our results suggested that health complications were found in women who self-medicated misoprostol for induced abortions after gestational ages greater than 6 weeks during the COVID-19 lockdown.
Keywords: Abortion, Misoprostol, Over-the-Counter Drug, Self-medication.
Unsafe abortions are very common in Pakistan and lead to many deaths. Women who opt for such abortions counter many complications. These are often recognized late and women reach hospitals in critical condition. Commonly encountered complications are severe hemorrhage, trauma to the genital tract, uterine perforation, and severe sepsis. Most of these complications are avoidable and can be treated successfully, however poor accessibility to health care and delays in seeking care are often the reasons for these catastrophic outcomes1.
Heavy bleeding may ensue from the genital tract in some cases and can jeopardize maternal health. Women are vulnerable in pregnancy due to physiological changes and bleeding may increase the chance of needing blood transfusion and treatment for correction of anemia which may not be readily available and accessible. In certain cases, heavy bleeding can lead to hysterectomy, and sepsis due to unsafe abortion which can lead to multi-organ failure. Surgical termination of pregnancy is therefore a procedure that needs training and is often not acceptable to women. Medical terminations however have an edge over their surgical counterparts because they are perceived to be safer. The medications needed for medical termination are available over the counter and can be dispensed with minimal instructions 2. During the COVID-19 lockdown in Pakistan, the inequalities in sexual and reproductive health were further exposed and women were unable to access reproductive healthcare facilities and seek clinic-based abortion care3,4.
The majority of women in the West terminate unwanted pregnancies medically5. It is considered safe and more acceptable; routine follow-up is not recommended provided the user understands the implications6. In Western countries, misoprostol is a regulated prescription drug and not available over the counter7. In Pakistan it is available over the counter therefore a medical prescription is therefore not needed. Women use this medication to terminate pregnancy and do not get checked to assess the feasibility of this drug for them8. This harmful practice leads to the medication being used without proper counseling for warning signs and at gestational ages not suitable for misoprostol use9. Being a tertiary care center, we came across many cases of self-administration of misoprostol during lockdown, leading to many complications. The objective of this study was to consider the problems of self-administration of misoprostol for miscarriage during the COVID-19 lockdown.
This was an observational study conducted at Abbasi Shaheed Hospital from 1st March to 30th Sep 2020. This study was undertaken to study the complications of self-consumption of misoprostol tablets during the lockdown period. Women who reported that they had consumed misoprostol tablets for termination of pregnancy without consulting a medical professional were included. Those who took the medication after consulting a medical professional were excluded. Also excluded were women with complications after misoprostol intake when prescribed by a medical professional and those who had undergone any surgical intervention after misoprostol consumption in any other health facility.
All participants gave written and informed consent on admission. On admission, detailed general, systemic, and obstetric examinations and routine investigations were done in all women. A proforma was used to collect the following data. A brief history regarding previous pregnancies, gestational age at which misoprostol tablets were taken, and reason for self-medication. Heavy bleeding (as defined by the women on presentation), anemia (hemoglobin less than 11gram/deciliter, as documented in the blood report done on admission), incomplete abortion (defined as products of conception visible in the uterine cavity, on the ultrasound done at the time of admission), missed abortion, (fetus visible but no fetal cardiac activity seen, on the ultrasound done at the time of admission). The need for blood transfusion, ruptured uterus, and ruptured ectopic pregnancy (on clinical examination later confirmed on surgery) was also documented.
Data were analyzed using SPSS version 23. Mean and standard deviations were calculated for the quantitative variables like maternal age and gestational age at administration. Frequencies and percentages were calculated for the qualitative variables like anemia, blood transfusion, heavy bleeding, shock, sepsis, ruptured ectopic pregnancy, and ruptured uterus (yes/no). A bivariable analysis was done to see the effect of gestational age at intake of misoprostol on the complications encountered, chi square test or Fischer’s exact test was applied taking a p-value of ≤ 0.05 as statistically significant.
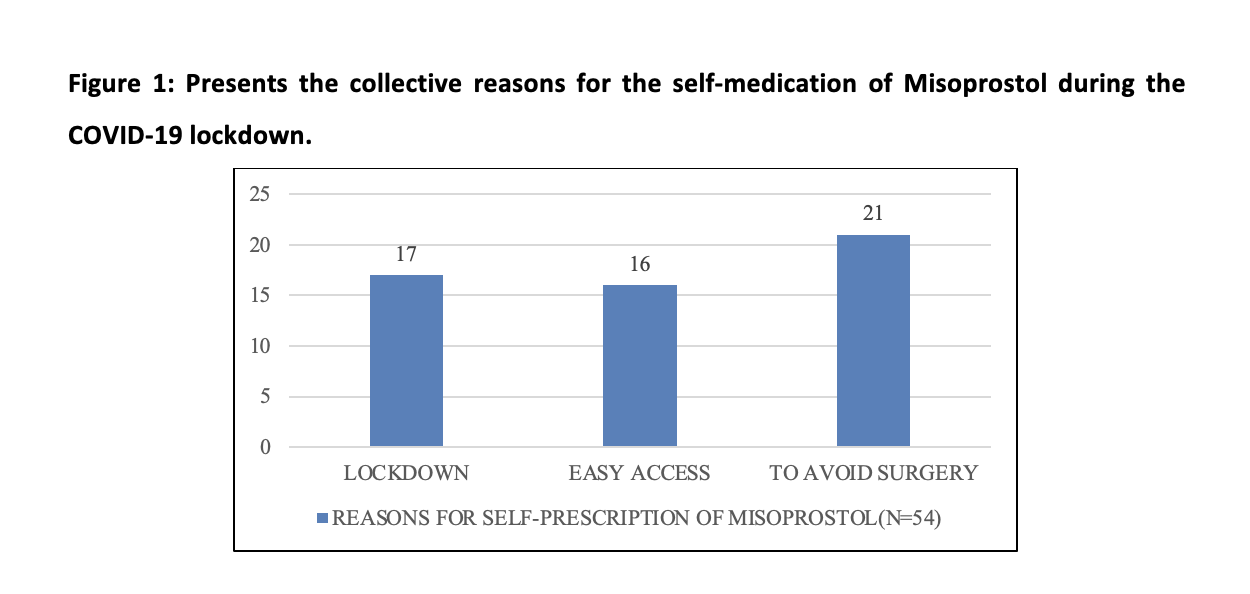
A total of 54 cases were studied. The mean age of the women was 31+/- 5 years. The mean gestational age at taking misoprostol was 7 +/- 2 weeks. The most common reason for taking misoprostol was to avoid surgery. (Table 1) The most common complication was anemia followed by incomplete abortion. There was one case of a ruptured uterus, the patient had previous 4 cesarean sections. One woman with a ruptured ectopic presented in a state of shock.
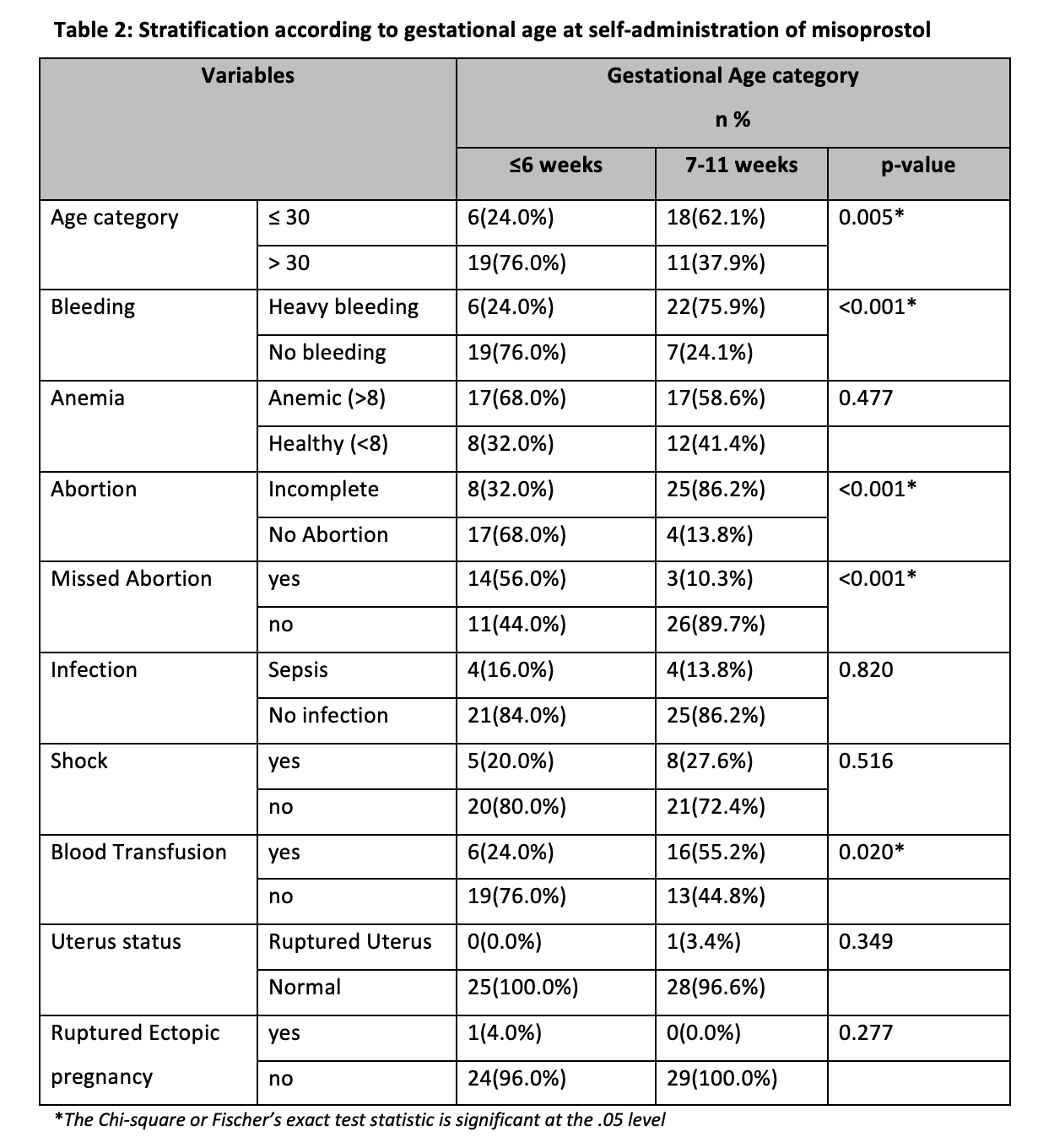
When stratified according to gestational age the complications were more common at gestational age greater than 6 weeks. (Table 2) Heavy bleeding (p˂0.001), blood transfusion (p=0.020), and incomplete abortion (p˂0.001) were significantly more common in women who used misoprostol at gestational ages greater than 6 weeks.
Misoprostol is famous as a single agent for medical abortion but is less successful than the combination of misoprostol and mifepristone10-11. The current standard and the Food and Drug Administration-approved regimen for medical abortion is 200 mg of mifepristone followed in 24–48 hours by 800 mcg misoprostol12. In our study, women came in with incomplete abortions and missed abortions but did not get a complete abortion. The effectiveness of misoprostol for termination is around 95%. These women may or may not have taken the complete dosage of the drug. Compliance with the protocol for drug administration is of utmost importance to achieve desirable results.
Heavy bleeding is much more likely in women who take misoprostol around 12 weeks and is less likely in women in earlier gestations. In our study, the heavy bleeding and the need for blood transfusion were significantly less likely in women who ingested misoprostol at earlier gestations. This is in agreement with previous studies on the topic 13-15. In our study, 48 out of 54 women just used misoprostol without any scan. This can be extremely dangerous in cases where the patient has an ectopic pregnancy and she takes misoprostol to abort it. In our study, 1 out of 54 women had this complication and she came in with ruptured ectopic. This is in contrast to the study from South America where no major adverse event was noted16.
Moreover, Misoprostol is contraindicated in women with previous cesarean sections and has been shown to cause uterine rupture in women. In our study a woman also presented with uterine rupture, she had previous 4 cesarean sections and did not want this pregnancy. She ingested a heavy dose and came in with torrential bleeding. These complications are not commonly encountered in Western countries because the access to medical care is significantly different, women are literate and abortion is not seen as a taboo topic17. Women who receive in-person follow up with a counselor are more likely to report a complete miscarriage. An ultrasound before administration of misoprostol can be helpful. It is not recommended that an ultrasound is done before giving misoprostol but women are always counseled to seek help if they develop complications and a pregnancy test needs to be repeated to ensure the pregnancy has been successfully terminated18.
WHO’s task-sharing guidelines recommend involving women in the management of combined mifepristone and misoprostol abortion regimens19. However, no such recommendations exist for misoprostol-only abortions. Our women mostly used a misoprostol-only regimen. Findings from a study suggest that perceptions of needing care are related to information or lack thereof, they received from drug sellers about potential complications and care-seeking needs20. Around 50% of women who reported that they needed some care had been warned by the drug dispensers that some complications could occur. In light of these findings, we conclude that misoprostol should be available only as a prescription drug. The policymakers should ensure that women are only given misoprostol when needed and after proper counseling and a follow-up is put in place for them to ensure continuity of care as it was proven to be of significance 21, 22, 23.
Our study is the first to assess the complications of self-administration of misoprostol for unwanted pregnancies during COVID-19 where health facilities are a stigmatized issue in Pakistan. The main limitation is its single-center design so the findings cannot be generalized to the whole population due to single-centered study and also not to higher socioeconomic groups of the city who may have a better understanding of the complications and are more likely to seek help before the situation deteriorates.
Misoprostol after gestational ages greater than 6 weeks was found associated with complications. There should be some restrictions on the over-the-counter availability of drugs used for medical termination of pregnancy. These should be administered only by healthcare providers in regions where women are unaware of complications and are less likely to access healthcare facilities for seeking care due to stigma.
We like to acknowledge hospital staff and doctors for their immense contribution.
The authors declared no conflict of interest.
The study used data records of the patients who came after taking misoprostol to terminate unwanted pregnancies. The study used retrospective data. Instead of formal ethics committee approval, the principles of the Helsinki Declaration were followed. Data was coded and confidentiality was ensured. The Head of the department granted permission for the study.
ZM, RI, and FA collected, analyzed, and interpreted the patient data and wrote the manuscript. SH, MM, and JM contributed to writing the manuscript.
- Sathar Z, Singh S, Rashida G, Shah Z, Niazi R. Induced abortions and unintended pregnancies in pakistan. Stud Fam Plann. 2014;45(4):471-491. doi: 10.1111/j.1728-4465.2014.00004.x.
- Bajwa SK, Bajwa SJS, Ghai GK, Singh N, Singh A, Goraya SPS. Medical abortion: is it a blessing or curse for the developing nations? Sri Lanka J Obstet Gynaecol. 2011;33(3):84–90. DOI:10.4038/sljog.v33i3.4015
- Abraish Ali1, Asad Ali Siddiqui1, Muhammad Sameer Arshad 1, Fizza Iqbal 1, Taha Bin Arif 1. Effects of COVID-19 pandemic and lockdown on lifestyle and mental health of students: A retrospective study from Karachi,Pakistan. Ann Med Psychol (Paris). 2021. doi: 10.1016/j.amp.2021.02.004.
- Hussein J. COVID-19: What implications for sexual and reproductive health and rights globally? Sex Reprod Health Matters. 2020;28(1):1746065. DOI: 10.1080/26410397.2020.1746065
- Tanne JH. Texas’s new abortion law is an attack on medical practice and women’s rights, say doctors. BMJ. 2021;374:n2176. doi: 10.1136/bmj.n2176.
- World Health Organization . Safe Abortion: Technical and Policy Guidance for Health Systems. Geneva: World Health Organization, 2012.
- Rossier C, Marchin A, Kim C, Ganatra B. Disclosure to social network members among abortion-seeking women in low- and middle-income countries with restrictive access: a systematic review. Reprod Health. 2021;18(1):114. doi: 10.1186/s12978-021-01165-0.
- Sarder A, Islam SMS, Maniruzzaman, Talukder A, Ahammed B. Prevalence of unintended pregnancy and its associated factors: Evidence from six south Asian countries. PLoS One. 2021;16(2):e0245923. doi: 10.1371/journal.pone.0245923.
- Schmidt-Hansen M, Cameron S, Lohr PA, Hasler E. Follow-up strategies to confirm the success of medical abortion of pregnancies up to 10 weeks’ gestation: a systematic review with meta-analyses. Am J Obstet Gynecol. 2020 ;222(6):551-563.e13. doi: 10.1016/j.ajog.2019.11.1244.
- Ngoc NT, Blum J, Raghavan S, et al. . Comparing two early medical abortion regimens: mifepristone + misoprostol vs. misoprostol alone. Contraception. 2011;83(5):410–417. doi: 10.1016/j.contraception.2010.09.002
- Jain JK, Dutton C, Harwood B, et al. A prospective randomized, double-blinded, placebo-controlled trial comparing mifepristone and vaginal misoprostol to vaginal misoprostol alone for elective termination of early pregnancy. Hum Reprod. 2002;17(6):1477–1482. doi: 10.1093/humrep/17.6.1477
- FDA Mifeprex® (mifepristone) tablets [drug insert]. New York (NY: ): Danco Laboratories; 2016.
- Niinimäki M, Mentula M, Jahangiri R, Männistö J, Haverinen A, Heikinheimo O. Medical treatment of second-trimester fetal miscarriage; A retrospective analysis. PLoS One. 2017;12(7):e0182198. doi: 10.1371/journal.pone.0182198.
- Jayaweera R, Powell B, Gerdts C, Kakesa J, Ouedraogo R, Ramazani U, Wado YD, Wheeler E, Fetters T. The Potential of Self-Managed Abortion to Expand Abortion Access in Humanitarian Contexts. Front Glob Womens Health. 2021; 2:681039. doi: 10.3389/fgwh.2021.681039.
- Bhandekar SS, Chauhan AR, Ambadkar A. Prospective Comparative Study of Oral Versus Vaginal Misoprostol for Second-Trimester Termination of Pregnancy. J Obstet Gynaecol India. 2018;68(6):456-461. doi: 10.1007/s13224-017-1076-2.
- Moseson H, Jayaweera R, Raifman S, Keefe-Oates B, Filippa S, Motana R, Egwuatu I, Grosso B, Kristianingrum I, Nmezi S, Zurbriggen R, Gerdts C. Self-managed medication abortion outcomes: results from a prospective pilot study. Reprod Health. 2020;17(1):164. doi: 10.1186/s12978-020-01016-4.
- Astbury-Ward E, Parry O, Carnwell R. Stigma, abortion, and disclosure—findings from a qualitative study. J Sex Med. 2012;9(12):3137–3147. doi: 10.1111/j.1743-6109.2011.02604.x
- Grossman D, Baum SE, Andjelic D, Tatum C, Torres G, Fuentes L, Friedman J. A harm-reduction model of abortion counseling about misoprostol use in Peru with telephone and in-person follow-up: A cohort study. PLoS One. 2018;13(1):e0189195. doi: 10.1371/journal.pone.0189195.
- World Health Organization Health worker roles in providing safe abortion care and post-abortion contraception. Geneva, Switzerland: World Health Organization, 2015.
- Stillman M, Owolabi O, Fatusi AO, Akinyemi AI, Berry AL, Erinfolami TP, Olagunju OS, Väisänen H, Bankole A. Women’s self-reported experiences using misoprostol obtained from drug sellers: a prospective cohort study in Lagos State, Nigeria. BMJ Open. 2020;10(5):e034670. doi: 10.1136/bmjopen-2019-034670.
- Moseson H, Keefe-Oates B, Jayaweera RT, et alStudying Accompaniment model Feasibility and Effectiveness (SAFE) Study: study protocol for a prospective observational cohort study of the effectiveness of self-managed medication abortion. BMJ Open 2020;10:e036800. doi: 10.1136/bmjopen-2020-036800
- Moseson H, Jayaweera R, Egwuatu I, et al. Effectiveness of self-managed medication abortion with accompaniment support in Argentina and Nigeria (SAFE): a prospective, observational cohort study and non-inferiority analysis with historical controls. Lancet Glob Health. 2022;10(1):e105-e113. doi:10.1016/S2214-109X(21)00461-7
- Mirian Z, AbdiShahshahani M, Noroozi M, Mostafavi F, Beigi M. Effect of intervention based on the 5A self-management model on the improvement of behaviors related to women’s reproductive health after legal abortion. Sci Rep. 2023;13(1):11316. doi: 10.1038/s41598-023-38521-y.
This is an open-access article distributed under the terms of the CreativeCommons Attribution License (CC BY) 4.0 https://creativecommons.org/licenses/by/4.0/