By Anum Sami 1, Raima Bashir 2, Kulsoom Fatima Rizvi 3
- Dental Administrator, Urban Dental Centre, Mississauga, Canada
- Oral Biology Department, Bahria University Dental College, Bahria University Health Sciences Campus Karachi
- Preventive and Community Dentistry Department, Bahria University Dental College, Bahria University Health Sciences Campus Karachi, Pakistan.
DOI: https://doi.org/10.36283/PJMD12-4/004
How to cite: Sami A, Bashir R, Rizvi KF. Assessing the Knowledge and Adherence of Dental Students to Cross-Infection Control Measures. Pak J Med Dent. 2023;12(4): 11-18. Doi: 10.36283/PJMD12-4/004
Background: Cross-infection control is extremely pivotal to halt the propagation of contiguous diseases amongst people as they pose a tremendously increasing disease burden on our health care system. Therefore, this study aimed to assess the knowledge and adherence to cross-infection control measures among dental students in public and private institutions in Karachi.
Methods: This descriptive study was performed among dental students of public and private sector dental colleges in Karachi from January 2020 – February 2020. The questionnaire assessed the knowledge and adherence of dental students toward cross-infection control protocols during their clinical rotations. The chi-square test was used to analyze the relationship between students’ knowledge and practice of cross-infection control measures.
Results: A total of 202 students participated in this study. The students demonstrated adequate knowledge of cross-infection control measures. However, the practice of wearing gloves was positive (98%) in contrast to the use of masks (79%), gowns (46%), and eyewear (13%). A statistically significant relation was seen in their knowledge and attitude toward hand hygiene. The immunization status of students from both government (72%) and private (88%) sectors raised concerns. Although students demonstrated good practice of measures to avoid transmission of contagious diseases (p=<0.001) apart from the use of environmental barrier (36%) (p=0.047) and disinfection (37%) of the working surface.
Conclusion: The overall knowledge of cross-infection control was satisfactory among dental students. Efforts are needed to improve the degree of compliance with recognized policies for improving the attitude of students regarding cross-infection measures.
Keywords: cross infection control, dental student, public and private sector, transmissible disease.
Infectious diseases have been a major public health problem and a global burden on healthcare systems. Cross infection is a term that expresses the transmission of infections from patient to health care provider/auxiliary staff, or from health care provider to their staff and similarly to patient either directly or by contaminating the clinical environment1. Dental Clinics are a potential source of cross-infection due to direct contact with blood, saliva, and handling of contaminated instruments with the body secretion. Needle stick injuries are also common if the contaminated instruments are not handled with care. The splattering and aerosols generated due to the functioning of dental instruments also assist in the propagation of infectious microbes and disease2,3. The control of cross-infection and cross-contamination have thus been a major concern in dentistry owing to constant exposure of infectious agents in the dental environment and the responsibility therefore lies on the health care professionals to follow a stringent cross-infection control routine in their practice for protection and preventing transmission of infectious diseases4. The cross-infection protocols recommended by the Occupational Safety and Health Administration (OSHA) for hospital and clinical practices apply the use of personal protective equipment for hands such as gloves, clothes, a white coat/apron, a mask to cover the nose, and eyewear to protect the eyes. Proper cleaning and disinfection of dental units and flooring and proper sterilization of all used dental equipment (motor and manual) by autoclave. Adequate disposal of disposal items like syringes, needles, cartridges, and patients’ contaminated materials (like cotton, gauze pieces, etc.)5,6. Cross-infection protocols must never be overlooked or ignored.
The discipline of infection control has experienced a renaissance during the last two decades which was stimulated by the emergence of the AIDS epidemic in the 1980s7. This, in turn, led to recommendations by the US Centers for Disease Control and Prevention (CDC) for more rigorous precautions concerning the prevention of Human Immunodeficiency Virus (HIV) transmission and following isolation precaution guidelines in healthcare settings7.
Dentists have the highest risk of acquiring cross-infection among health professionals; with 2.5- to 6-fold higher experience of hepatitis B among dentists8. Dental Practices in Pakistan have been identified as a potential risk factor in transmission of infectious diseases especially Hepatitis B & C, tuberculosis, and HIV predominantly due to poor level of infection control practice and lack of awareness among unqualified practitioners and auxiliaries9. It is the dental staff and students in particular who are prone to these detriments due to their inadequate knowledge and the nature of work which also play a role in the dissemination of these diseases10.
The level of knowledge and practice of infection control measures was poor among dental students while the attitude was positive, but greater compliance was needed11. However, in Karachi, Pakistan favorable results were found on knowledge regarding infection control among dental students but emphasized the need to transfer that knowledge into daily practice12-13. Among all factors needle stick injury is the most common source of accidental exposure among dental students14 and their poor knowledge, attitude, and practices regarding infection control especially among senior dental professionals as compared to house officers and junior professionals15–16.
Although there is enough scientific support for knowledge and awareness of dental health care professionals regarding infection control, research comparing the practicing behavior of public and private dental students is limited. Therefore, the objective of this study was to obtain comprehensive information regarding OSHA guidelines corresponding to cross-infection among the study population and assess its application by adherence in their daily practice. The study also aimed to compare the level of knowledge regarding infection control practices among dental students in public and private sector teaching hospitals in Karachi.
This descriptive, cross-sectional research study was executed among third and final-year undergraduate dental students from Jan to Feb 2020. The sample size extracted via the Online Open Epi Software v3.0 sample size calculator was n=250 keeping the confidence level at 95% with a 5% margin of error. However, about 202 students’ proforma were found to be complete and thus processed for data analysis. The response rate was 80.8%. The research data was obtained from the following public and private dental colleges of Karachi: Dow University of Health Sciences (DUHS), Karachi Medical and Dental College (KMDC), Altamash Institute of Dental Medicine (AIDM), and Bahria University Medical & Dental College (BUMDC) by non-probability convenience sampling technique.
Dental students of the 3rd and 4th-year BDS program, both genders, who have been allocated in the clinical department rotations in OPDs, with at least 6 months’ experience in patient handling, and showing a willingness to participate in the research study were included in the study. However, dental students in preclinical years (1st and 2nd years) and having less than 6 months of clinical experience along with Postgraduate trainees, General Dental Practitioners, and those students unwilling to participate in the study were excluded. All the participants enrolled in the study signed an informed consent form.
Prior permission to collect data was obtained from the respective institutional heads while the study was approved by the Ethics Review Committee of BUMDC reference # ERC 13/2020. A self-administered closed-ended questionnaire comprising 23 questions adapted from a previous study14 and with slight modifications was employed for data collection.
The collected data was analyzed by SPSS version 23. The descriptive data was represented using percentages and frequencies. Correlation among knowledge, attitudes, and practice between public and private sector institutes was assessed by the Chi-Square test and Fisher Exact Test. A p-value of ≤ 0.05 was considered to be significant.
In this study, a total of 202 completed questionnaires were received from students belonging to government and private institutions. The results of students’ knowledge and attitudes are tabulated.
Figure 1 displays the knowledge and attitude of students toward personal protection protocol. A very positive result was seen regarding the use of gloves by both government 73 (96%) and private students 124 (98.4%) in contrast to other personal protection gear which was notably low. The use of masks was more frequently practiced in private colleges n=106/126 (84%) as compared to government n=53/76 (70%).
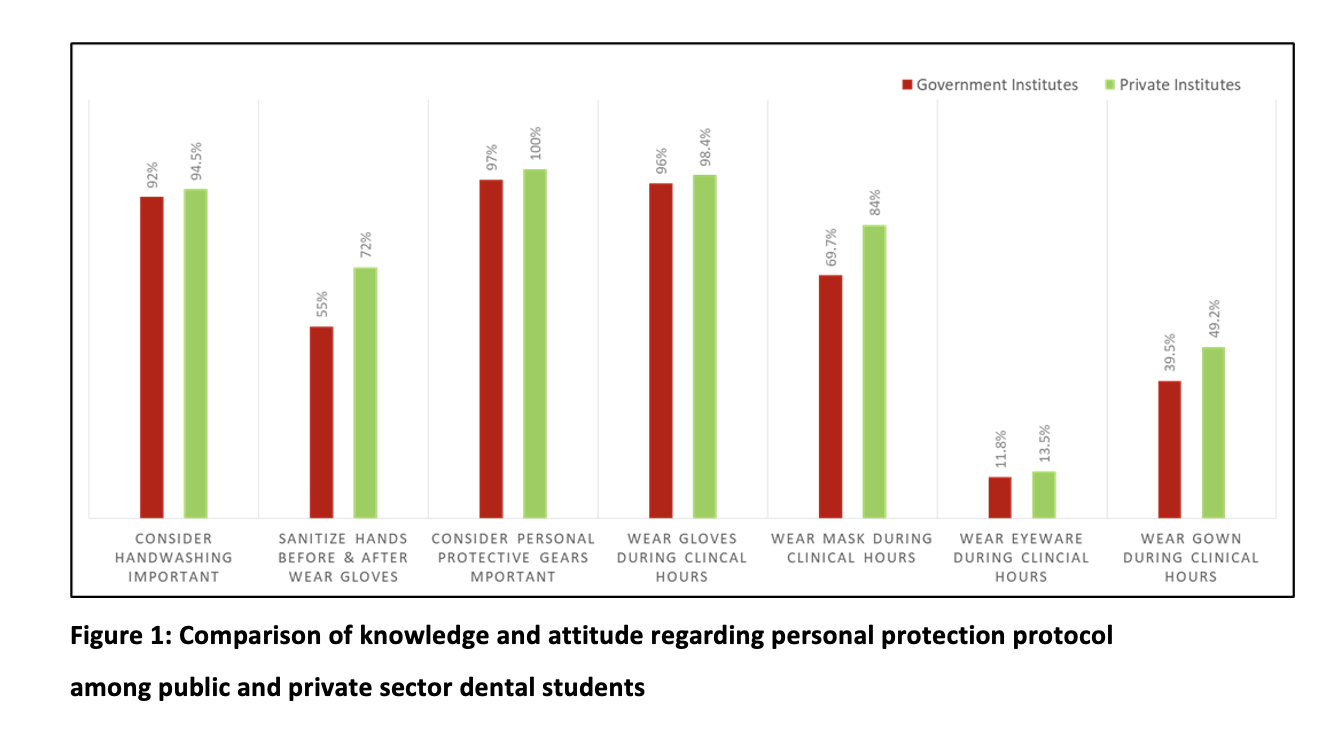
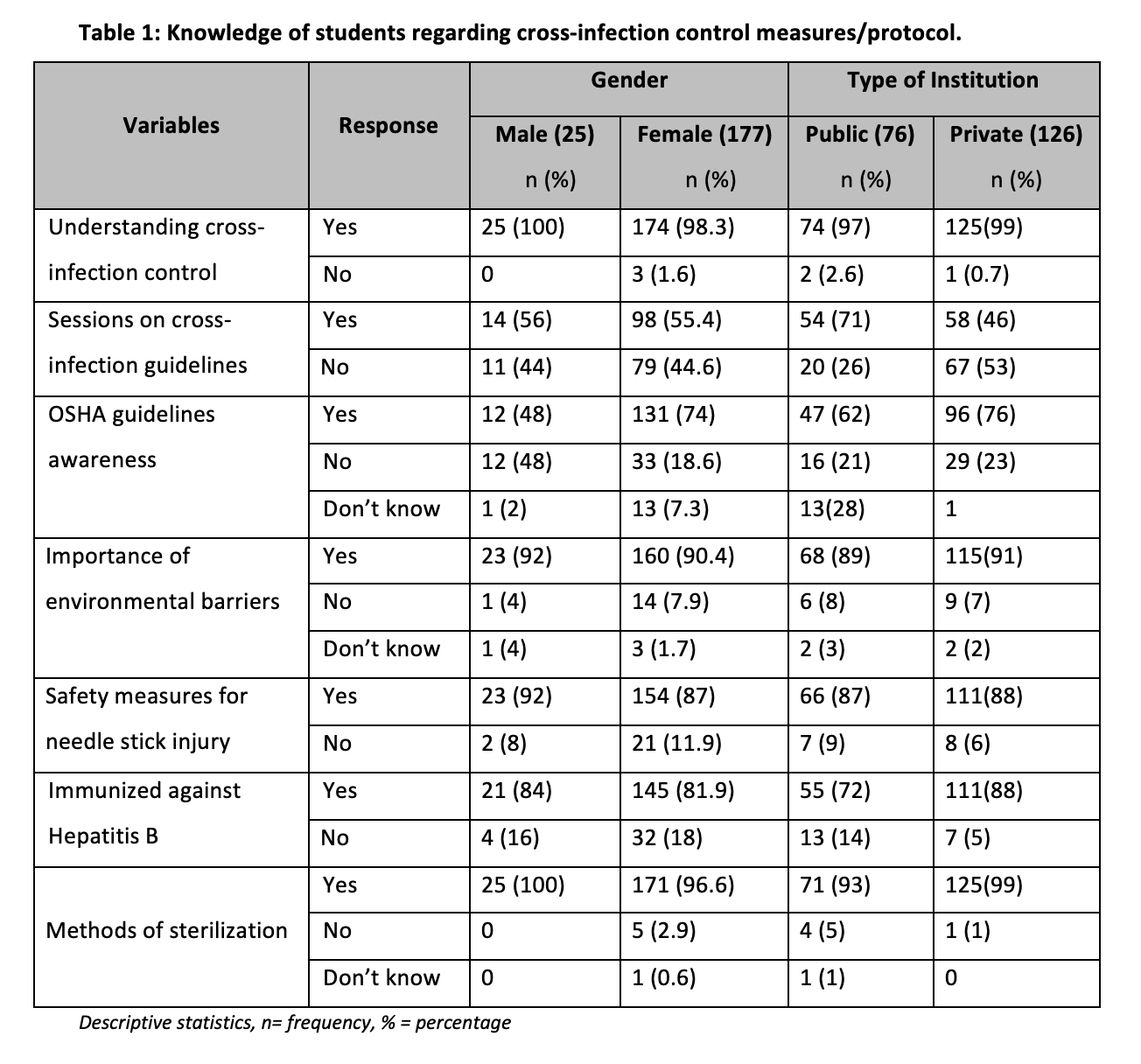
Table 1 depicts the knowledge and attitude of students to cross-infection control measures. It is noteworthy to mention that nearly all of the students were aware of the term cross infection control n= 199/202. Knowledge regarding cross-infection control as well as cross-infection practices was found to be better in males as compared to females. A good percentage of students 54 (71%) from government institutions had attended an educational session cross infection in contrast to private institutions 58 (46%). Nearly one-third of all the students 59 (29%) were unaware of standard precaution guidelines by OSHA despite being part of their curriculum. Also, the immunization status against Hepatitis B of students in a public institute was 16/29 (55%).
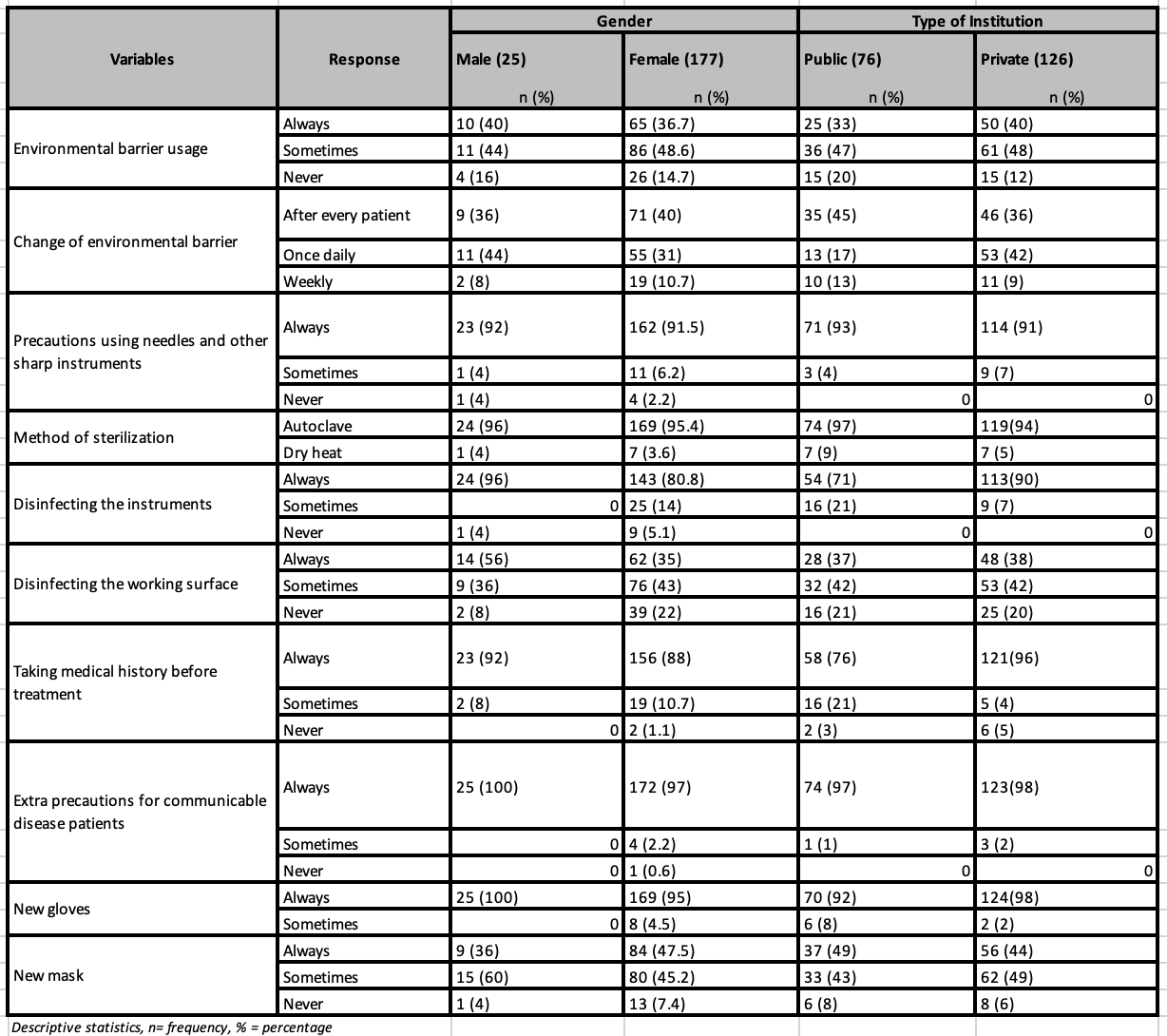
The protocol of changing gloves for every patient was routinely followed among all the students 194 (98%) while contradictory results were seen among students regarding changing masks for every patient 93 (46%). Practices such as the use of new gloves for every patient 100% / 98%, taking extra precautions against communicable diseases 100% / 98% and needle stick injuries 92% / 91%, always disinfecting instruments 96% / 90% and history take as precautionary measures 92% / 96% against the spread of diseases were higher in males as compared to females and amongst students of private institutes in comparison to public institutes (table 2).
Table 2: Attitude, and adherence of students regarding cross-infection control measures/ protocol.
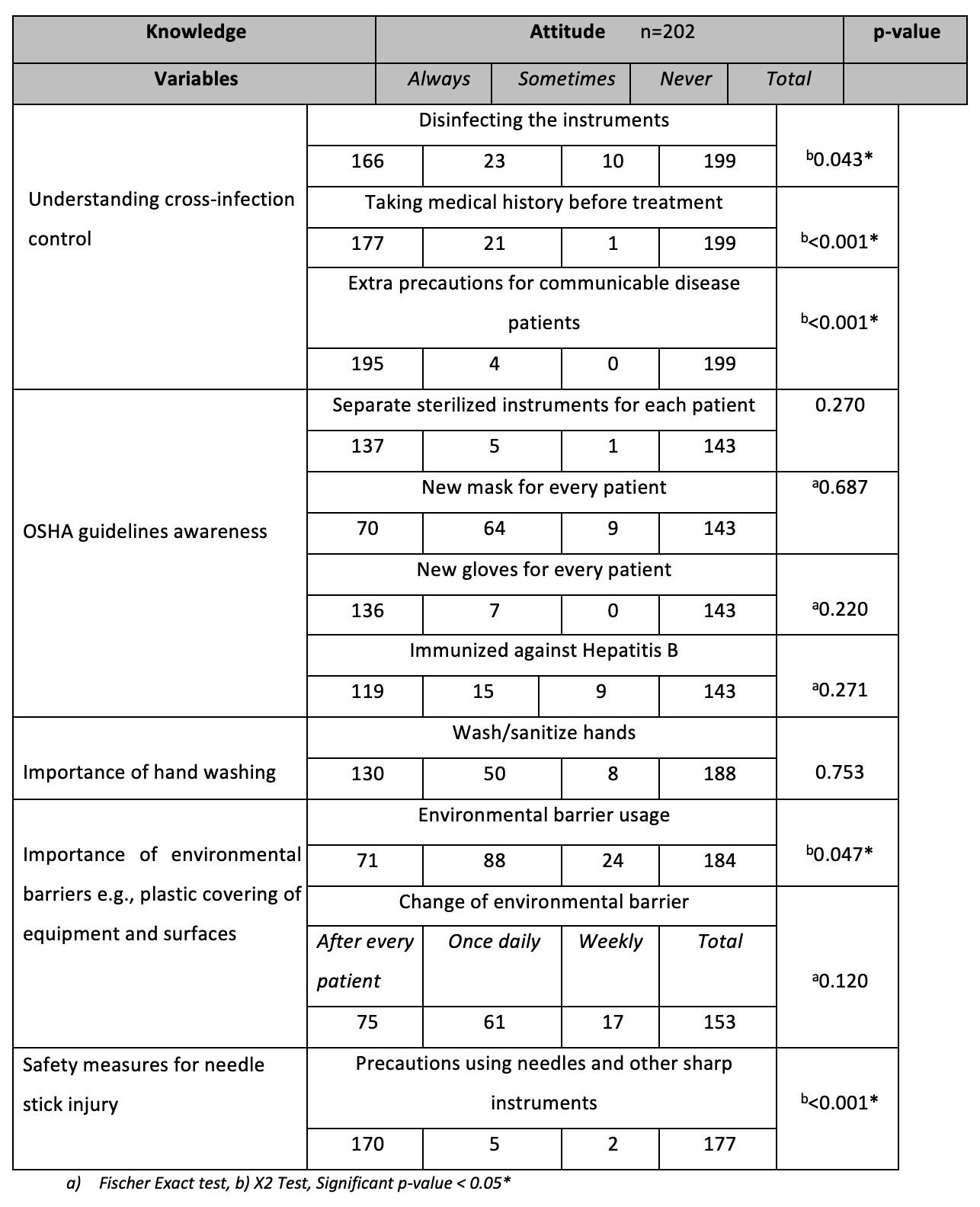
The practice of frequent hand wash was highest among dental students. This also proved to be statistically significant (p=0.003*) when associated with their knowledge of hand hygiene. The students showed varying responses to the use of environmental barriers but whenever practiced, it was strictly changed after every patient. When this was correlated with their knowledge, a statistically significant(p=0.047*) relationship was found. The disinfection of instruments was regularly practiced 167 (83%) and showed a significant result (p=0.016*) when correlated with their knowledge of cross-infection control. A thorough medical history taking was carried out by the majority of students 179/202 (88.6%) and extra precautions were taken for patients with transmissible diseases. This practice was also found to be statistically significant (p=0.001*) (Table 3).
Table 3: Correlation between knowledge and attitude of dental students
Most infectious diseases that colonize the oral cavity and respiratory tract, including the novel coronavirus, can be transmitted in a dental clinic. The high percentage of affected people worldwide increases the chance of them attending dental clinics, which, in turn, poses a risk of exposure to and contraction by dentists and other staff members17. This study assessed the knowledge of students and their corresponding practicing behavior concerning cross-infection control from government and private hospital settings. The overall knowledge of cross-infection control was satisfactory among dental students and similar findings were reported by other studies in Pakistan12,13. The contributing factors could be curriculum emphasis and educational seminars conducted during their graduate program. Also, professional guidelines are set by the institute and regulatory bodies. Dental students are typically taught to adhere to these guidelines, ensuring they are well-informed about the best practices in infection control.
Upon comparing our findings regarding the use of personal protective gear with other studies, both similarities and differences were observed. In our study, the percentage of participants wearing gloves was 98%, which aligns with a study conducted in Saudi Arabia17. However, variations were noted in the utilization of masks, gowns, and eyewear. In our study, the respective percentages were 79%, 46%, and 13%, whereas in a study by Halavani et al, they were 93%, 98%, and 60.7% 18. These discrepancies indicate a lack of sufficient understanding regarding the importance of eye protection, considering the potential transmission of diseases through aerosols and blood. Nevertheless, other studies conducted in Pakistan demonstrated similar compliance with personal protection against infections12,13. This underscores the necessity to enforce rules and regulations, with educational institutions ensuring strict adherence to protocols by students.
Hands serve as the primary reservoir for numerous pathogens, highlighting the utmost significance of hand hygiene in preventing infections. Handwashing is considered a fundamental and effective method for infection prevention19. In response to the COVID-19 pandemic, the World Health Organization (WHO) has recommended a comprehensive handwashing approach, involving washing hands with soap and water for a minimum of 20 seconds, followed by the use of alcohol-based hand rub (ABHR) for visibly soiled hands 20.
In our present study, we found that students were well aware of the importance of hand hygiene, with an impressive awareness rate of 94%. Their adherence to the standard hand hygiene protocol was 72% in private schools and 55% in government schools, as observed in the study by Waheed Tahir et al. conducted in a government setup, which reported a compliance rate of 74%13. In contrast, Marium et al. reported a higher compliance rate of 94% with hand hygiene in a private institute19. Similarly, a study conducted in India by Bommireddy et al. demonstrated a compliance rate of 59% in handwashing practices among dental practitioners21. While a majority of students in our study changed gloves between patients, it was noted that not all consistently followed proper handwashing protocols, as also reported by Noura A. et al17. This indicates a lack of institutional emphasis and guidelines regarding hand hygiene. To address this concern, we recommend reinforcing proper handwashing techniques among students and considering placing educational posters in handwashing areas, which would serve as useful reminders.
Although the participants in our study believed environmental barriers such as plastic wrapping for dental units were important the practice was not very consistent, with only 33% in government and 39% in private. Similar results were seen for the disinfection of the working surface. This finding also concurs with past studies12,13, 19, 22. However, studies by Halawani et al. and Chang HC et al. show significantly improved compliance with the environment disinfection protocol post-COVID-19 18, 23. This suggests that the basics of infection control should be overemphasized by continuous lectures and training sessions.
Our study revealed excellent knowledge and attitudes of students towards handling and disposing of needles. Also, a thorough medical history and patients with communicable diseases were treated according to OSHA guidelines. This finding is by previous studies13,15,24. However, the immunization status of students was found to be 72% and 88% in government and private institutes respectively. Similar results were seen in previous studies in the subcontinent12,13,25. A study conducted by Elagib MFA et al. in Sudan and Saudi also reported a low percentage of post-HBV serology26. This finding suggests that the institute should make hep B vaccination proof mandatory for all students and a booster dose before starting clinical practice/rotations. A study by Alharbi et al. found that 93.1% of their undergraduate students were vaccinated due to this regulation followed by the college 27.
Nonetheless, this study involved both government and private colleges therefore it displays more variability. The dissimilarity in the attitude of participants may be due to a person’s own beliefs, thoughts, and behavioral aspects. The lack of resources and adherence to strict institutional policy, particularly in the government sector could also play a role.
One of the limitations of this study was the method used to assess the practice of infection control guidelines which is based on students’ subjective self-assessment. Also, the generalizability of the findings is constrained by the convenience sample of dental students and the limited sample size. Another limitation was the absence of qualitative data due to the limited time available during data gathering. This was a multi-center study (being carried out in private and public sector dental colleges of Karachi), which will help us elucidate the level of knowledge and practice regarding cross-infection control procedures among undergraduate dental students. It will help the institutes identify the awareness and practice of cross-infection protocols being practiced at their institutes and will also help to learn and share information with other institutes for the best interest of their students and patients’ safety. It will also allow the conduct of regular workshops to enhance and improve awareness among future dentists.
The students from both public and private institutes reported good knowledge indicating that cross-infection control guidelines are outlined by OSHA. Lack of adherence to the guidelines at certain levels spotlights the need for an evaluation program as a means of assuring compliance with recognized policy in clinical practice. This will help create a safe environment for both the practitioners and the patients and help build patients’ trust in doctors and healthcare facilities.
We would like to acknowledge the honest participation of all the participants and the public and private institutes’ faculty who were part of this research study for their immense cooperation.a
Authors declare no conflict of interest
The study was approved by the Ethics Review Committee of BUMDC reference # ERC 13/2020.
Written and verbal consent was taken by all participants before handing out the questionnaire.
AS was responsible for the literature research, concept, and design of the study. AS and RB performed data collection and manuscript writing. RB conducted a statistical analysis and reviewed the final manuscript. KFR supervised the research work and provided final proofreading.
- Ibrahim NK, Alwafi HA, Sangoof SO, Turkistani AK, Alattas BM. Cross-infection and infection control in dentistry: Knowledge, attitude, and practice of patients attended dental clinics in King Abdulaziz University Hospital, Jeddah, Saudi Arabia. Infect. Public Health. 2017;10(4):438-445.
- Bains R, Tikku AP, Bains VK, Verma P. Knowledge, attitudes, and practices of dental patients toward cross-infection and economic implications given covid-19: An online survey.Adv. Oral Res. 2021;12(1):95-102.
- Ahmed MA, Jouhar R, Adnan S, Ahmed N, Ghazal T, Adanir N. Evaluation of patient’s knowledge, attitude, and practice of cross-infection control in dentistry during COVID-19 pandemic. Eur J Dent. 2020;14(1):1-6. DOI: 10.1055/s-0040-1721295
- Volgenant CM, De Soet JJ. Cross-transmission in the dental office: does this make you ill? Oral Health Rep. 2018;5:221-228.
- Das G, Samejo I, Ahmed S, Jabeen B, Shaikh MI, Mushtaque K. Cross infection control in private dental practice in Karachi, Sindh. Professional Med. J. 2019;26(08):1354-1358.
- Ratnayake D et al. Awareness of the risk of cross-infection and infection-control measures among patients attending University Dental Hospital, Peradeniya, Sri Lanka. J Investig Clin Dent 2018;1:1-4.
- Siegel JD, Rhinehart E, Jackson M, Chiarello L. Guideline for isolation precautions: preventing transmission of infectious agents in health care settings. J. Infect. Control. 2007;35(10):S65-164. DOI: https://doi.org/10.1016/j.ajic.2007.10.007
- Mahboobi N, Agha‐Hosseini F, Mahboobi N, Safari S, Lavanchy D, Alavian SM. Hepatitis B virus infection in dentistry: a forgotten topic. J. Viral heat. 2010;17(5):307-316. DOI: https://doi.org/10.1111/j.1365-2893.2010.01284.x
- Ahmed H. Methods of sterilization and monitoring of sterilization across selected dental practices in Karachi, Pakistan. J Coll Physicians Surg Pak Oct. 2015;10:713-716.
- Alharbi G, Shono N, Alballaa L, Aloufi A. Knowledge, attitude and compliance of infection control guidelines among dental faculty members and students in KSU. BMC Oral Health. 2019;19:1-8. https://doi.org/10.1186/s12903-018-0706-0)
- Singh A, Purohit BM, Bhambal A, Saxena S, Singh A, Gupta A. Knowledge, attitudes, and practice regarding infection control measures among dental students in Central India. J Dent Educ. 2011;75(3):421-427. DOI: https://doi.org/10.1002/j.0022-0337.2011.75.3.tb05055.x4
- MF, Hussain A, Maqsood A. Knowledge, attitude and practice concerning infection control measures among dental health care providers of
Dow University of Health Sciences. Pak. Oral Dent. J. 2014; 34(3):452-456. - Tahir MW, Mahmood A, Abid A, Saadullah M, Sajid. Knowledge, attitude, and practices of cross infection control among dental students of Punjab, Pakistan. Pak J Med Health Sci. 2018;12: 238-242
- Assiri KI, Naheeda, Kaleem SM, Ibrahim M, Alam T, Asif SM. Knowledge, attitude, and practice of infection control among dental students in King Khalid University, Abha. J Int Oral Health. 2018;10:83-87.
- Mohiuddin S, Dawani N. Knowledge, attitude and practice of infection control measures among dental practitioners in the public setup of Karachi, Pakistan: a cross-sectional survey. J Dow Univ Health 2015;9(1):3-8.
- Mustafa EA, Humam AK, Al-Mosuli TA. Evaluation of dental assistant awareness concerning infection control policy of blood-borne diseases. J Int Dent Med Res. 2015; 8(1):21-24.
- Noura A. AL-Essa, Manal A. AlMutairi. To what extent do dental students comply with infection control practices, The Saudi Journal for Dental Research. 2017;8(1-2):67-72. ISSN 2352-0035. https://doi.org/10.1016/j.sjdr.2016.10.003.
- Halawani R, Aboalshamat K, Alwsaidi R, Sharqawi S, Alhazmi R, Abualsaud Z, Alattallah A, Alamri M. Awareness and Practices of Dental Students and Dentists Regarding Infection Control in Prosthodontic Clinics. Open Dent J. 2020;14(1):184-190. DOI: https://doi.org/2174/1874210602014010184
- Qamar MK, Shaikh BT, Afzal A. What do the dental students know about infection control? A cross-sectional study in a teaching hospital, Rawalpindi, Pakistan. Bio Med Res. Int. 2020:1-5 DOI: https://doi.org/10.1155/2020/3413087
- Siddharta A., Pfaender S., Vielle N.J., Dijkman R., Friesland M., Becker B., Yang J., Engelmann M., Todt D., Windisch M.P. Virucidal Activity of World Health Organization–Recommended Formulations Against Enveloped Viruses, Including Zika, Ebola, and Emerging Coronaviruses. Infect. Dis. 2017;215: 902–906. DOI: 10.1093/indices/jix046
- Bommireddy VS, Pachava S, Sanikommu S, Vinnakota NR, Talluri D, Ghanta BK. Infection control measures among dental practitioners in a Southern state of India: A cross-sectional study. J Indian Assoc Public Health Dent. 2016;14: 302-307. DOI:https://doi.org/10.4103/2319-5932.187178
- Shah FA, Alanazi AO, Alrawili YK, Alanazi YM. Knowledge and attitudes towards infection control protocols among the students of Al-Jouf University in Saudi Arabia. J. Hosp. Med. 2018;71(6):3328-3331
- Cheng HC, Chang YJ, Liao SR, Siewchaisakul P, Chen SL. The impact of COVID-19 on knowledge, attitude, and infection control behaviors among dentists. BMC Oral Health. 2021;21(1):584. DOI: 10.1186/s12903-021-01946-w.
- El-said, C.; Dadras, O.; Musumari, P.M.; Ono-Kihara, M.; Kihara, M. Infection Control Knowledge, Attitudes, and Practices among Students of Public Dental Schools in Egypt. Int. J. Environ. Res. Public Health 2021, 18, 6248. DOI: https:// doi.org/10.3390/ijerph18126248
- Akanksha R, Vikas K, Jitendra M, Shalini J, Panna L, Satyavir S. Assessment of knowledge, attitude, and practices toward prevention of hepatitis B infection among medical students in a high-risk setting of a newly established medical institution. J Lab Physicians 2018;10(04): 374-379. DOI: https://doi.org/10.4103/JLP.JLP_93_18
- Elagib MFA, Baldo SMH, Tawfig A, Alqarni MA, Ghandour IA, Idris AM. Knowledge, attitude, and practice regarding infection control measures among dental students during the COVID-19 pandemic. Arch Environ Occup Health. 2022;77(6):455-467. DOI: 10.1080/19338244.2021.1931796.
- Alharbi G, Shono N, Alballaa L, Aloufi A. Knowledge, attitude and compliance of infection control guidelines among dental faculty members and students in KSU. BMC Oral Health. 2019;19(1):1-8. DOI: https://doi.org/10.1186/s12903-018-0706-0
This is an open-access article distributed under the terms of the CreativeCommons Attribution License (CC BY) 4.0 https://creativecommons.org/licenses/by/4.0/