By Haifa Saquib Baqai1, Muhammad Bilal Bashir2, Imtiaz Ahmed3
- Oral Biology Department, Hamdard University, Karachi, Pakistan
- Oral Biology Department, Fatima Jinnah Dental College, Karachi, Pakistan
- Orthodontics Department, Dow University of Health Sciences, Karachi, Pakistan
DOI: https://doi.org/10.36283/PJMD12-4/005
How to cite: Baqai HS, Bashir MB, Ahmed I. Analysis of Root Angulation of Maxillary Central Incisor Using Cone Beam Computed Tomography (CBCT) Pak J Med Dent. 2023;12(4): 19-24. Doi: 10.36283/PJMD12-4/005
Background: Variance in anatomical morphology is influenced by the axial inclination of the tooth. When looking at the axial tilt of the crown, it’s common to assume that it follows the same axis as the root. This study aims to use Cone Beam Computed Tomography (CBCT) to determine the root angulation correlation in maxillary central incisors.
Methods: This cross-sectional observational research was performed at Dow University of Health Sciences (DUHS). The CBCT scans of patients who matched the inclusion criteria were done by skilled radiography technicians and primary investigators on ROTOGRAPH EVO 3D. For statistical analysis, one-way ANOVA was utilized to examine the Root Angulation (RA) with different root positions. p-value <0.05 was considered significant.
Results: This study examined n=152 CBCT images. Mean age was 27.2 + 5.9 years, with 32(42.1%) men and 44(44.1%) females. Buccal subtype I was most prevalent (59, 38.8%) in maxillary central incisors, while buccal subtype III was least common (5, 3.3%). The root angulations varied significantly between root location classifications (p=0.007). These were intermediate root location (14.9 2.6 degrees) and buccal subtype III (14.28 2.25 degrees). The palatal root type had the least angle (3.73 1.5 degrees).
Conclusion: The buccal root position was shown to be the most common root location. Buccal subtype I was by far the most common. Buccal subtype III and middle root location had the maximum root angle. The palatal root position had the smallest angle.
Keywords: Alveolar bone, Cone Beam Computed Tomography, Incisors.
The first thing a person notices about someone is their smile and a proportionate smile line requires balance and symmetry¹. The anterior teeth play a major role in aesthetics, particularly the central incisors². The maxillary central incisors are the most noticeable teeth and hence the most obvious dentition in the dental arches. Earlier research showed that the Collum angle varies amongst individuals with altered kinds of malocclusion. Differences in the anatomic structures of the maxillary central incisors can disturb both the management and the retention stage of orthodontic treatment. Thus, it is significant to identify the collum angle and its difference in such circumstances for effective planning and application of treatment management.
The location and position of the maxillary central incisor have a dominant role in aesthetics, phonetics, and mastication3. The variations in maxillary anterior teeth have been observed between genders and races⁴⁻⁶. Many studies have been done to elucidate the different methods to get the good dimension for the perfect smile, specifically considering factors such as the maximum amount of gingival display amount of buccal corridors⁷⁻⁹ and the long axis of deviation and impact of the midline¹⁰⁻¹².
The standardized changes in the proportion of the incisors have a powerful impact on a person’s attractiveness using computer-manipulated photographs¹³. Modification in width-to-length ratios was most recognized within the range of 75 to 85%, and variation in tooth to tooth proportion has 50 to 74% of pleasant appearance ¹⁴. Hence, the three-dimensional (3D) position and placement of the maxillary incisor are key factors in achieving the desired result during dental treatment ¹⁵.
The axial inclination of a tooth plays an important role in the variation of anatomical morphology. While observing the axial inclination of the crown, it is typically presumed that the crown follows the same axis as that of a root. However, studies have shown that the axial inclination of the crown can significantly vary from the longitudinal axis of the root. CBCT has signified its accuracy regarding root angulation, implant placement, and crown root angulation measurement worldwide, whereas panoramic investigation in such conditions can result in overestimation of implant length, magnification of bone size, and wrong measurement of angulation. The Collum angle which is the angle of the crown root of the maxillary central incisors is very essential for patients who are going to have orthodontic treatment and who are undergoing a dental implant placement procedure ¹⁵.
Maxillary central incisors have the widest mesiodistal diameter out of all the anterior teeth present in the maxillary arch, but the smallest convex labial surface is present. However, the crown surface of the labial aspect is quite smooth. The distal and mesial curvature crest on this aspect provides the contact points between adjacent incisors. The current study aimed to determine the correlation of root angulation in maxillary central incisors using Cone Beam Computed Tomography (CBCT).
This cross-sectional observational research was performed at Dow University of Health Sciences (DUHS), Karachi from August 2020 to February 2021. Participants were chosen from Dow University of Health Sciences affiliated institutes and hospitals (DUHS). The Institutional Review Board gave ethical approval for the study (REF: IRB1378/DUHS/Approval/2019). The convenience sampling strategy was utilized to identify study participants who reported to the dental outpatient department and were prescribed CBCT scans. This study examined n=152 CBCT images. Healthy individuals between 18 and 30 years old with a CBCT image of good quality were included. Participants with tooth decay, pathology of the anterior soft tissues, more than 4mm of alveolar bone loss at the cementoenamel junction, teeth that have been restored or broken, treated with orthodontics, image artifacts, and patients with a systemic illness.
The CBCT scans of patients who matched the inclusion criteria were done by the radiography section of DUHS. The CBCT data was collected by a skilled radiography technician and the primary investigator on the ROTOGRAPH EVO 3D. 3D planner version 2.0 2018 villa SM 2018 was used to analyze the CBC.
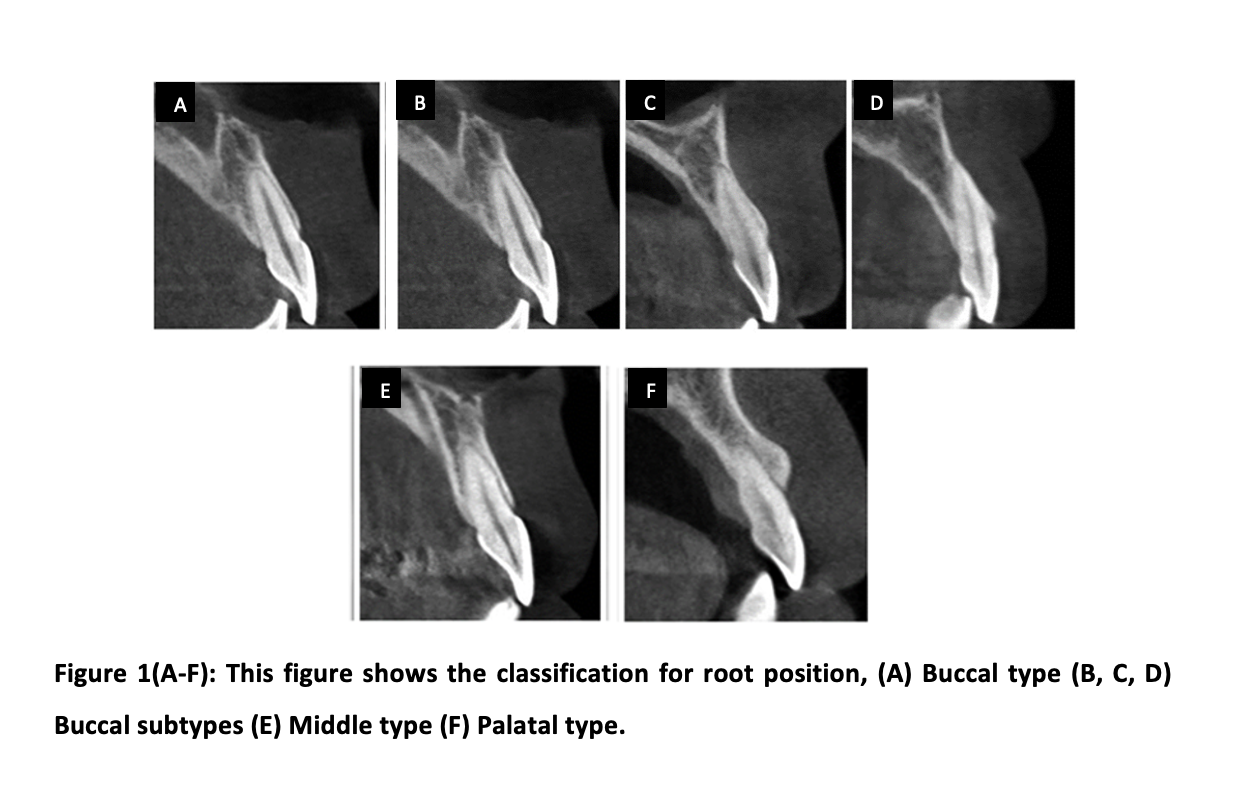
The root position was visually assessed. The root apex was thought to be the most crucial criterion when placing a tooth in a class or subtype according to categorization. Root angulation is determined by the tooth’s long axis and the alveolar bone angle. In a cross-sectional view, the long axis of a tooth is the line connecting the incisal edge and the root apex. The long axis of an alveolar bone is a line that runs parallel to the corresponding alveolar bone from top to bottom. In terms of bone, the angle created by these two axes (the long axis of the tooth and the long axis of the bone) is known as root angulation. Figure 1 shows the classification of the root position that has been used in our study for reference.
SPSS v21 was used for statistical analysis. The Shapiro-Wilk test was used to determine the normality of the data. Parametric tests were utilized since the data was regularly distributed. To compare the RA data with different root locations, a one-way ANOVA was used.
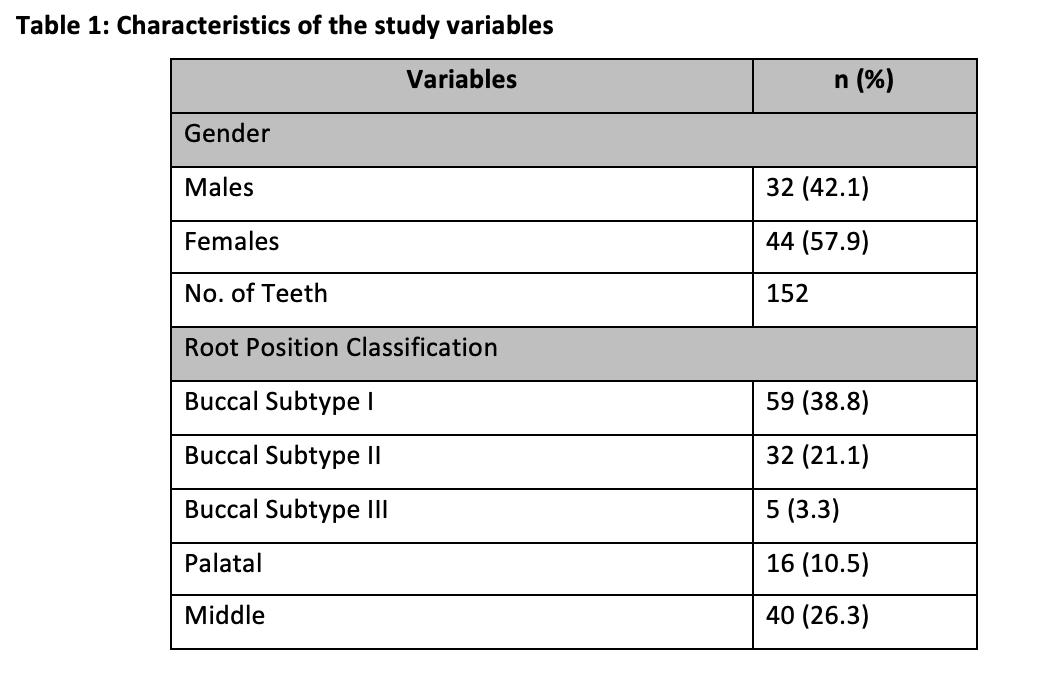
In this study, a total of 152 CBCT images were observed. The mean age of the study participants was 27.2 ± 5.9 years, with CBCT images of 32 (42.1%) males and 44(57.9%) females. The total number of teeth observed was 152. Buccal subtype I was the most frequent type (N=59, 38.8%) observed in the maxillary central incisors, while buccal subtype III was the least observed type (N=5, 3.3%) among patients (Table 1).
A one-way ANOVA compared the root angulation values to the root position. There was a significant variation in root angulations in different root location classifications (p-value=0.007). The intermediate type of root location (14.9 ± 2.6 degrees) and buccal subtype III (14.28 ± 2.25 degrees) had the largest mean angle. The palatal type of root location had the least angle (3.73 ± 1.5 degrees). (Table 2)
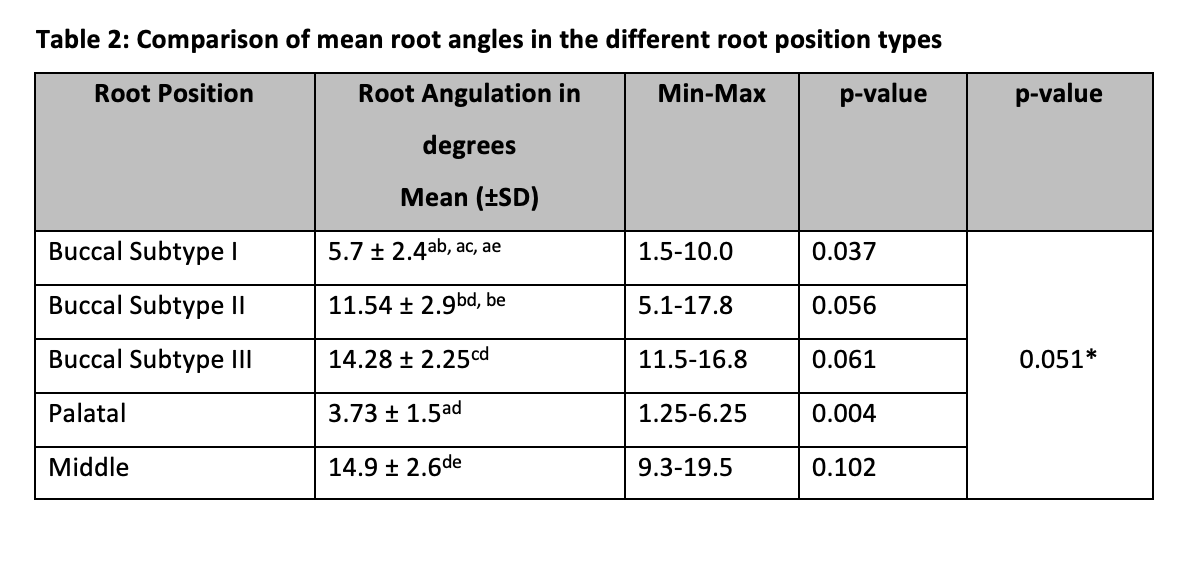
*A significant difference between the mean root angles of different root positions after applying the Post hoc test. ab: buccal subtype I vs II; ac: buccal subtype I vs III; ad: buccal subtype I vs palatal; ae: buccal subtype I vs middle; bc: buccal subtype II vs III; bd: buccal subtype II vs palatal, be: buccal subtype II vs middle; cd: buccal subtype III vs palatal; ce: buccal subtype III vs middle; de: palatal vs middle.
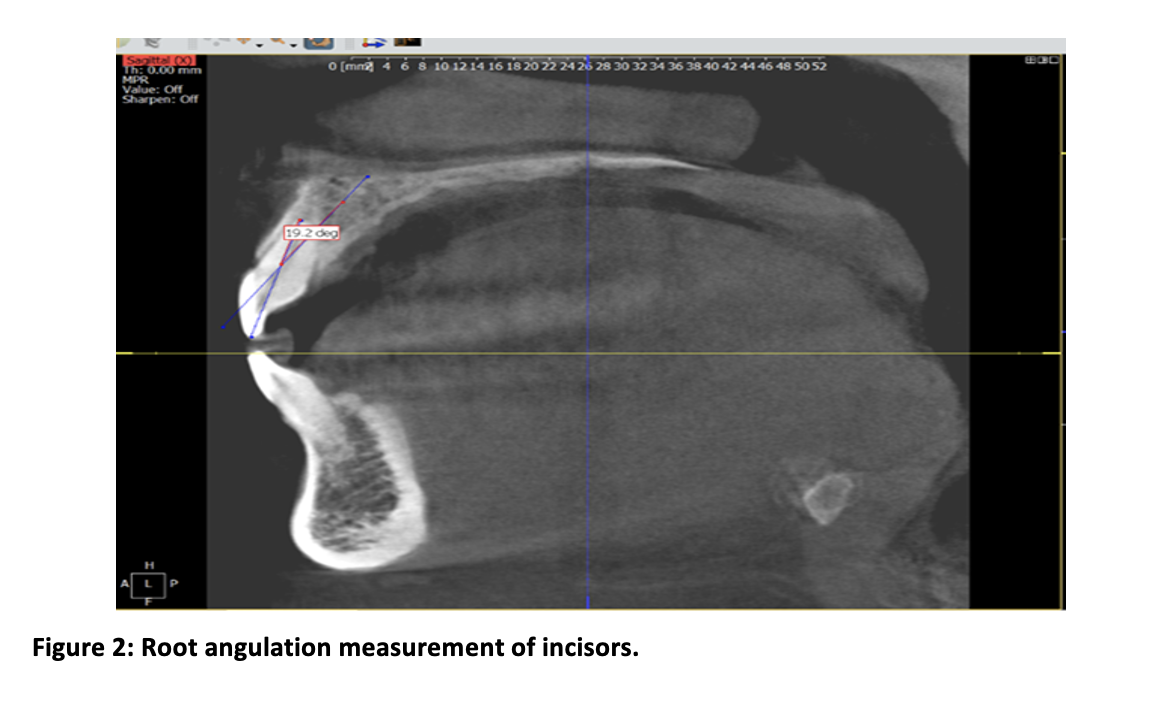
In Figure 2, the measurement of root angulation was done by measuring the angle between the axis of the tooth and the alveolar bone. The line passing through the lowest point of the incisal edge to the highest point of the root apex in the cross-sectional image is considered as the long axis of the tooth. The point where these two axes (the long axis of the tooth and the long axis of the bone) bisect each other, forms an angle that is defined as root angulation with respect to the bone.
The axial inclination of a tooth plays a significant role in the discrepancy of anatomical morphology¹⁶⁻¹⁷. While noticing the axial inclination of the crown, it is classically acknowledged that the crown follows the same axis as that of a root¹⁸. However, researchers have shown that the axial inclination of the crown can considerably vary from the longitudinal axis of the root¹⁹. CBCT has shown its accuracy regarding root angulation, implant placement, and crown root angulation measurement worldwide, whereas panoramic investigation in such circumstances can result in overestimation of implant length, magnification of bone size, and wrong measurement of angulation²⁰⁻²¹.
The current study was undertaken to assess the root angulation of the maxillary central incisor using CBCT. The classification of Jung et al. was used to determine the root position within the alveolar bone²². Furthermore, root angulation was also measured in the central incisor in the said classification. This study observed that the buccal type was the most prevalent, followed by the middle-type root position. These findings are by several other studies that determined that the maxillary central incisor has good buccal bone coverage. Lou et al. observed 170 images and observed that 78.8% of the incisors were buccally placed. Their study did not further classify the buccal type into subtypes²³.
In this study, we identified teeth as buccal subtypes I, II, and III. The root of the buccal subtype I is completely covered by the buccal bone, making it appropriate for both IIP and orthodontic therapy. The buccal subtype I prevents root resorption and bone loss by providing excellent bone covering to the root of the maxillary central incisor. Buccal subtype I accounted for 38.8% of maxillary central incisors, the highest percentage in this study. These results are consistent with Jung et al., who found that buccal subtype I is the most common type in maxillary central incisors²².
Xu et al. studied the sagittal root position and its clinical significance by using CBCT. They observed 934 maxillary central incisors and observed that 95.4% (N=891), 4.4% (N=41), and 0.2% (N=2) were classified as buccal, middle, and palatal, respectively ²⁴. Among the 891 buccal-type incisors, the subtypes I, II, and III accounted for 47.5% (N=423), 44.2% (N=394), and 8.3% (N=87). In this study, we observed a greater number of teeth falling in the palatal and middle type classification than the study conducted by Kan et al., who observed that 13% of the teeth account for the middle type of root position ²⁵. Another study conducted on CBCT images of maxillary central incisors also concluded that 58.8% of maxillary central incisors are inclined buccally. Kong et al. observed 120 scans for evaluating the maxillary aesthetic zone and concluded that the buccal type of root positioning was the most prevalent (81.1%) ²⁶ which is similar to this study. Another study done by Yang et al. shows maximum numbers of buccally placed incisal roots (97.1%) with thin facial bone coverage. In this study, such morphological features are matched with buccal subtype II, which was 21.1% of the total sample size²⁷.
Suweera et al. studied root axis angulation and alveolar bone axis with SRP and anterior arch forms. Roots closer to the buccal bone (class I) were most prevalent in the maxillary central incisor and first premolar. Roots engaging palatal plates were not observed in their study. They further elaborate that the anterior arch form can give an idea about the root angulation of teeth because they observed that root angulation and alveolar bone axis decrease as the inter canine depth of the arch becomes smaller. Our results show similarity with their results in terms of root positions and angulations²⁸.
Mengru Shi et al. studied root angulation of maxillary central and lateral incisors for evaluation of implant placement as per hard and soft tissue indices via CBCT and stereolithography (STL). The average angle for the maxillary central incisor was 15 degrees. They explored that root angulation of lateral incisor in males was on average 4 degrees greater than central incisor. Root angulation showed a tendency with an increase in age which can be due to bone resorption²⁹.
Patients are not aware of the significance of CBCT, proper knowledge should be delivered by the health professionals. This investigation is technique-sensitive, and technical persons and skills are lacking to interpret CBCT images, therefore, proper training should be provided to operators. A greater sample size can give a better idea of position and angulation among the population.
The study found that the buccal root position was the most prevalent. In the buccal position, subtype I was the most prevalent. The highest root angle was observed in the buccal subtype III and middle root position. The least angle was observed in the palatal root position.
The authors would like to acknowledge the Dow University of Health Sciences for facilitating the study.
The authors declared no conflict of interest.
The participants were explained the steps involved in the procedure and consent was obtained.
HSB was the primary author, collected the data, did the interpretation and analysis, and wrote the manuscript. IA, topic selection, and supervision. MBB re-analyzed the data for inter-examiner reliability. All the authors contributed to the write-up and final revision of the manuscript.
- Machado AW, McComb RW, Moon W, Gandini Jr LG. Influence of the vertical position of maxillary central incisors on the perception of smile esthetics among orthodontists and laypersons. Journal of esthetic and restorative dentistry. 2013;25(6):392-401. DOI: 10.1111/jerd.12054
- Menezes EBC, Bittencourt MAV, Machado AW. Do different vertical positions of maxillary central incisors influence smile esthetics perception? Dental press journal of orthodontics. 2017;22:95-105. DOI: 10.1590/2177-6709.22.2.095-105.oar
- Khalid Z, Iqbal K, Khalid S, Riaz A, Jan A. Comparison of collum angle of maxillary central incisors in different incisor relationships. J Coll Physicians Surg Pak. 2020;30(05):471-475. DOI: 10.29271/jcpsp.2020.05.471
- Shrestha P, Paudel S, Neupane M, Lamba S. Anterior Tooth Width Measurements among Patients in a Tertiary Hospital of Nepal: A Descriptive Cross-sectional Study. JNMA: Journal of the Nepal Medical Association. 2020;58(226):396. DOI: 10.31729/jnma.4994
- Gillen RJ, Schwartz RS, Hilton TJ, Evans DB. An analysis of selected normative tooth proportions. International journal of prosthodontics. 1994;7(5).
- Lavelle C. Maxillary and mandibular tooth size in different racial groups and different occlusal categories. American journal of orthodontics. 1972;61(1):29-37. DOI: 10.1016/0002-9416(72)90173-x
- Krishnan V, Daniel ST, Lazar D, Asok A. Characterization of the posed smile by using a visual analog scale, smile arc, buccal corridor measures, and modified smile index. American journal of orthodontics and dentofacial orthopedics. 2008;133(4):515-523. DOI: 10.1016/j.ajodo.2006.04.046
- Nimbalkar S, Oh YY, Mok RY, Tioh JY, Yew KJ, Patil PG. Smile attractiveness related to buccal corridor space in 3 different facial types: A perception of 3 ethnic groups of Malaysians. The Journal of Prosthetic Dentistry. 2018;120(2):252-256. DOI: 10.1016/j.prosdent.2017.10.021
- Sikandar H, Adil S. Perception of an esthetical smile about the buccal corridor. Pakistan Orthodontic Journal. 2018;10(2):87-90.
- Correa BD, Bittencourt MAV, Machado AW. Influence of maxillary canine gingival margin asymmetries on the perception of smile esthetics among orthodontists and laypersons. American Journal of Orthodontics and Dentofacial Orthopedics. 2014;145(1):55-63. DOI: 10.1016/j.ajodo.2013.09.010
- Kan J, Rungcharassaeng K, Roe P, Mesquida J, Chatriyamuyoke P, Caruso JM. Maxillary central incisor-incisive canal relationship: a cone beam computed tomography study. Am J Esthet Dent. 2012;2(3):180-187.
- Matsumura T, Ishida Y, Kawabe A, Ono T. Quantitative analysis of the relationship between maxillary incisors and the incisive canal by cone-beam computed tomography in an adult Japanese population. Progress in orthodontics. 2017;18(1):1-6. DOI: 10.1186/s40510-017-0181-1
- Wolfart S, Thormann H, Freitag S, Kern M. Assessment of dental appearance following changes in incisor proportions. European journal of oral sciences. 2005;113(2):159-165. DOI: 10.1111/j.1600-0722.2005.00206.x
- Gulizio MP, Agar JR, Kelly JR, Taylor TD. Effect of implant angulation upon retention of overdenture attachments. Journal of Prosthodontics: Implant, Esthetic and Reconstructive Dentistry. 2005;14(1):3-11.DOI: 10.1111/j.1532-849X.2005.00005.x
- Nguyen T, Cevidanes L, Cornelis MA, Heymann G, de Paula LK, De Clerck H. Three-dimensional assessment of maxillary changes associated with bone anchored maxillary protraction. American Journal of Orthodontics and Dentofacial Orthopedics. 2011;140(6):790-798. DOI: 10.1016/j.ajodo.2011.04.025
- Rafi ST QT. Comparison of Collum Angle of Maxillary Central Incisor in High Angle and Low Angle Patients. JPDA. 2021
- Castro IO, Gribel BF, de Alencar AHG, Valladares-Neto J, Estrela C. Evaluation of crown inclination and angulation after orthodontic treatment using digital models. Journal of Orofacial Orthopedics/Fortschritte der Kieferorthopädie. 2018;79(4):227-234. DOI: 10.1007/s00056-018-0136-2
- Cong A, Massaro C, Ruellas ACdO, Barkley M, Yatabe M, Bianchi J, et al. Dental Long Axes using Digital Dental Models Compared to Cone‐Beam Computed Tomography. Orthodontics & Craniofacial Research. 2021. DOI: 10.1111/ocr.12489
- Nandeshwar N, Banerjee S, Shenoy U, Akhare P, Hazarey A, Karia H, et al. Comparative Evaluation Of Collum Angle Of Maxillary Central Incisor In Patients With Angles Class I, Class Ii Division 1 And Class Ii Division 2 Malocclusions–A Cephalometric Study. Contemporary Research Journal of Medical Sciences. 2018;2(1):1-8.
- Vandenberghe B. The digital patient–Imaging science in dentistry. Journal of dentistry. 2018;74:S21-S6. DOI: 10.1016/j.jdent.2018.04.019
- Elangovan B, Srinivasan B, Kailasam V, Padmanabhan S. Comparison of the collum angle of incisors and canines in skeletal malocclusions–A CBCT study. International Orthodontics. 2020;18(3):468-79. DOI: 10.1016/j.ortho.2020.06.006
- Jung Y-H, Cho B-H, Hwang JJ. Analysis of the root position of the maxillary incisors in the alveolar bone using cone-beam computed tomography. Imaging science in dentistry. 2017;47(3):181-187. DOI: 10.5624/isd.2017.47.3.181
- Lau SL, Chow J, Li W, Chow LK. Classification of maxillary central incisors—implications for immediate implant in the esthetic zone. Journal of Oral and Maxillofacial Surgery. 2011;69(1):142-153. DOI: 10.1016/j.joms.2010.07.074
- Xu D, Wang Z, Sun L, Lin Z, Wan L, Li Y, et al. Classification of the root position of the maxillary central incisors and its clinical significance in immediate implant placement. Implant dentistry. 2016;25(4):520-524. DOI: 10.1097/ID.0000000000000438
- Kan JYK, Rungcharassaeng K, Deflorian M, Weinstein T, Wang HL, Testori T. Immediate implant placement and provisionalization of maxillary anterior single implants. Periodontology 2000. 2018;77(1):197-212. DOI: 10.1111/prd.12212
- Kong H-J. A study on sagittal root position of maxillary anterior teeth in Korean. Journal of Dental Rehabilitation and Applied Science. 2020;36(2):88-94.
- Yang G, Hu W, Cao J, Liu D. Measurement of sagittal root position and the thickness of the facial and palatal alveolar bone of maxillary anterior teeth. Zhonghua kou qiang yi xue za zhi= Zhonghua kouqiang yixue zazhi= Chinese journal of stomatology. 2013;48(12):716-720.DOI:10.3760/cma.j.issn.1002-0098.2013.12.004
- Petaibunlue S, Serichetaphongse P, Pimkhaokham A. Influence of the anterior arch shape and root position on root angulation in the maxillary esthetic area. isd. 2019;49(2):123-130. DOI: 10.5624/isd.2019.49.2.123
- Shi M, Wang X, Zeng P, Liu H, Gong Z, Lin Y, et al. Analysis of the sagittal root angle and its correlation with hard and soft tissue indices in anterior teeth for immediate implant evaluation: a retrospective study. BMC Oral Health. 2021;21(1):494. DOI: 10.1186/s12903-021-01848-x
This is an open-access article distributed under the terms of the CreativeCommons Attribution License (CC BY) 4.0 https://creativecommons.org/licenses/by/4.0/