By Hafsa Mahida, Sarwat Memon, Ali Kazi
AFFLIATIONS:
Department of Orthodontics, Ziauddin College of Dentistry, Ziauddin University, Karachi Pakistan.
DOI: https://doi.org/10.36283/PJMD11-2/010
ORCID iD: 0000-0001-7870-5180
How to cite: Mahida H, Memon S, Kazi A. Variables Associated with Clinical Decision Making in the Treatment of Class I Malocclusion Patients. Pak J Med Dent. 2022;11(2): 57-64. doi: 10.36283/PJMD11-2/010
Background: To achieve treatment goals in orthodontics, the decision to extract or not extract premolars meets with debate. This includes cephalometric findings and study-cast analysis as influencing factors. This research aimed to identify variables that aid in clinical decision-making in the treatment of Class 1 malocclusion patients.
Methods: This was a retrospective study conducted on pre-treatment records of Class I patients. All patients had a Class I dental and skeletal malocclusion. A sample of n=80 patients was included (40 extraction cases, 40 non-extraction). Cephalometric values and study-cast analysis for tooth-arch size discrepancy were performed and binary logistic regression was applied to run the univariate and multivariable analysis to investigate the association of different variables with extraction and non-extraction treatment. Odds ratio (OR) and 95% confidence intervals were reported and p <0.05 was considered statistically significant.
Results: Univariate logistic regression showed that mandibular and maxillary crowding (p<0.001), overjet (p<0.001), SNGo (p= 0.01), nasolabial angle (NL) (p= 0.02), lower anterior facial height (LAFH) (p= 0.03) and upper lip in plane (ULE) (p= 0.05) had a significant association with the extraction and non-extraction groups. Hence, final multivariable logistic regression revealed that crowding (p< 0.01, 0.02), overjet (p= 0.009) and NL angle (p= 0.56) showed significant difference between the groups treated with and without extraction (p <0.05).
Conclusion: The level of crowding in both the arches, the incisal overjet, and the nasolabial angle aid in the clinical decision-making for Class I malocclusion patients in choosing an extraction or non-extraction plan.
Keywords: Extraction; Non-Extraction; Class I; Malocclusion; Patients; Orthodontics.
Improved facial appearance is one of the fundamental reasons why patients choose orthodontic treatment. The concept of ideal facial appearance principally determined by the patient’s profile and the application of two principle treatment methods whether to perform extractions or not has been an exceptionally questionable issue in the literature of orthodontics. There are mainly two approaches to treat skeletal class 1 malocclusion- dental extraction and arch expansion to gain space. These two approaches are directed at the correction of tooth size versus arch size discrepancy, which is a common problem in class 1 malocclusion1. The approach to extract commonly involves the removal of premolars. To plan an orthodontic treatment with extraction or not has been a widely discussed topic in the study of orthodontics. The trends of the extraction have varied greatly over time. Based on Angle’s opinion that all 32 teeth could be accommodated in the existing arches, conventionally non-extraction treatment was the preferred approach1-3.
To diagnose and form a treatment plan of an orthodontic patient, a set of variables including the estimations of cephalometric and model analysis alongside the age and sex of a patient must be assessed thoroughly by an orthodontist, which will ultimately aid in reaching a decision3-5. Various other factors such as congenitally missing or previously extracted teeth, restorations, and periodontal health are highly significant in decision making. After taking the entirety of the fore-mentioned factors into account, the treatment plan is set up and the requirement for an extraction or a non-extraction plan is advocated. In the diagnosis of a Class 1 patient, numerical values of the variables are highly significant and having a thorough knowledge of these variables will help in forming treatment predictors by distinguishing the use of one therapeutic method over the other, thereby leading to swift decision making. To distinguish which variables, affect the orthodontist’s choice if it is to opt for the extraction or not, it is imperative to comprehend that a treatment outcome of a patient with certain characteristics treated in one manner will vary compared to those treated by another. An orthodontist is then ultimately led by these characteristics to reach a choice of treatment, acknowledged as confounding variables5,6.
With the conventional approach falling to relapse, extractions gained popularity for several reasons with a degree of crowding being the chief reason to pursue extraction of the premolars. Furthermore, Tweed concluded that extractions enhanced and lead to more harmony in facial profile and greater stability7. Konstantonis et al. in their research concluded certain variables should not be neglected while making an orthodontic treatment plan, some of which are the lower crowding, lower lip to E-plane, upper crowding, and overjet8. With treatment planning and decision-making varying from case to case and approaches of clinicians being diverse, it would seem necessary to suggest sound clinical indicators which determine the need for extractions. Hence, the outcome of this research may expedite the treatment planning procedure for patients with Class I malocclusion. The purpose of this study was to identify variables that aid in clinical decision-making in the treatment of Class 1 patients.
This was a retrospective, cross-sectional comparative study conducted on pre-treatment records of patients with a Class I malocclusion which was selected at random from the Orthodontic Department, Ziauddin College of Dentistry from 2014 to 2019. A request for waiver of the ethics review committee was put forward to the university for the process as there was no patient contact, no new tests were done and patient confidentiality was maintained. The request was accepted and waiver no. 2951220HMOM was granted by the Committee. To eliminate selection or proficiency bias, all the included records were evaluated under the supervision of two trained orthodontists of the department.
All patients were males and females of Pakistani origin with a full dentition (excluding the third molars) who presented with a Class I dental and skeletal malocclusion. The selected cases had no history of any cleft, dentofacial deformity, or syndrome nor had they received any previous orthodontic treatment. Using the Open Epi online sample size calculator, assuming a prevalence of 57% for non-extraction cases in class 1 patients at the power of 80% and confidence level of 95%, a sample size of a total of 80 patients was calculated. Therefore, records of 40 patients in each group (extraction and non-extraction group) were included in this study.
The subjects were divided into two groups: 40 were treated without extraction whereas the other 40 were treated by extracting the four first premolars. Radiographs were taken by the department of radiology of Ziauddin Hospital. Lateral Cephalometric films were taken using the Planmeca Proline XC X-ray unit through constant exposure of 9ma, 70kvp for 18sec. The cephalometric landmarks were identified and were evaluated by two trained orthodontists working in the department of orthodontics of Ziauddin College of Dentistry.
Cephalometric landmarks were identified as per the definitions in the orthodontic literature. From these landmarks, various cephalometric measurements were derived which included SNA, SNB, and ANB angles; Nasion perpendicular to point A, Nasion perpendicular to Pog. Witt’s analysis, SN-GoGn angle, FMA, lower anterior-facial height, UI-SN angle, IMPA, nasolabial angle, and relationship of upper and lower lips concerning the E and S planes as depicted in Figure 1 and Figure 2.
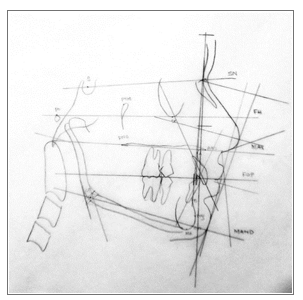
Figure 1: A cephalometric tracing of a Class I case with a non-extraction plan.
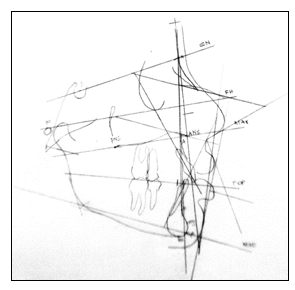
Figure 2: A Cephalometric tracing of a Class I case with an extraction plan was decided.
The overjet, overbite, upper and lower dental midlines, and maxillary and mandibular tooth size-arch length discrepancies were calculated on dental casts using a digital Vernier caliper (0-150 mm ME00183; Dentaurum, Pforzheim, Germany). This was performed with an accuracy of 0.02 mm and a reliability of 0.01 mm as per the manufacturer’s specifications.
Data were analyzed through STATA version 14. In order to summarize the categorical variables, frequencies with proportions were employed whereas mean and standard deviation was used for continuous variables. Binary logistic regression was applied to run the univariate and multivariable analysis to study the association of different independent variables (from cephalograms and dental casts) with extraction and non-extraction treatment outcomes. Odds ratio (OR) and 95% confidence intervals were reported. All tests were two-sided and p-value <0.05 was considered statistically significant. Independent variables were also checked for multicollinearity amongst them using Pearson’s correlation. A high correlation was considered for values greater than 0.8.
A total of n=80 patients were included in this research, 40 in extraction and 40 in the non-extraction group. The mean age of patients was found to be 17.91±4.93 years, a median of 17 years and ranging from 11 years to 38 years. The male to female ratio was 1:3. Among the males, 11 (55.0%) were extraction cases, whereas 29 (48.3%) of the females were in the extraction group (p-value 0.61) (Table 1).
Table 1: Descriptive analysis based on patient characteristics and clinical characteristics.
|
Patients’ Characteristics |
Extraction group
(n=40) |
Non-extraction group (n=40) |
| Frequency (n) (%) | Frequency (n) (%) | |
| Age categories (in years) | ||
| 11 to 14 | 15(62.5) | 9(37.5) |
| 15 to 17 | 9(47.4) | 10(52.6) |
| 18 to 21 | 10(52.6) | 9(47.4) |
| 22 to 38 | 6(33.3) | 12(66.7) |
| Gender | ||
| Male | 11(55.0) | 9(45.0) |
| Female | 29(48.3) | 31(51.7) |
| Clinical Characteristics | ||
| Mean ± SD | Mean± SD | |
| SNA (degree) | 80.7±3.3 | 81.1±3.4 |
| SNB (degree) | 78.1±3.1 | 78.5±3.6 |
| ANB (degree) | 2.5±1.2 | 2.7±1.0 |
| NA to Point A (mm) | -0.01±4.1 | -1.6±4.2 |
| NA to Pog (mm) | -4.2±4.4 | -6.3±7.0 |
| Wits (mm) | 0.4±3.4 | 0.5±2.4 |
| SNGo (degree) | 33.0±7.2 | 29.1±5.5 |
| FMA (degree) | 24.5±7.5 | 24.5±5.3 |
| LAFH (mm) | 56.7±2.4 | 59.8±7.8 |
| UISN (degree) | 111.0±5.3 | 108.8±9.6 |
| IMPA (degree) | 98.4±8.0 | 100.0±8.9 |
| ULS Plane (mm) | 0.8±1.9 | 0.6±2.5 |
| LLS Plane (mm) | 3.0±1.7 | 2.6±3.1 |
| ULE Plane (mm) | -2.1±2.6 | -3.4±3.2 |
| LL to E plane (mm) | 0.8±2.9 | -0.1±3.4 |
| Overjet (mm) | 5.0±2.1 | 3.0±1.7 |
| Overbite (mm) | 4.5±1.8 | 3.8±3.0 |
| Midline Lower (mm) | 1.0±0.9 | 0.7±0.8 |
| Midline Upper (mm) | 1.5±1.8 | 1.1±1.1 |
| Maxillary Crowding (mm) | 4.0±1.7 | 2.3±1.4 |
| Mandibular Crowding (mm) | 6.8±2.5 | 2.7±1.5 |
| NL Angle (degree) | 98.0±13.2 | 104.2±9.1 |
Univariate logistic regression in Table 2 shows that mandibular and maxillary crowding, overjet, SNGo, NL angle, LAFH and ULE plane had a significant association with the treatment groups (extraction and non-extraction). None of these variables were found to have multicollinearity among them. Hence, a final multivariable logistic regression model was run and it revealed that mandibular and maxillary crowding (p= 0.001, 0.02), overjet (p= 0.009) and NL angle (p= 0.56) showed a significant difference between the groups treated with and without extraction.
Table 2: Univariate binary logistic regression to study the orthodontic factors associated with extraction/non-extraction treatment groups.
| Extraction Treatment a | ||
| Independent Variables | Unadjusted OR | 95% CI |
| Age Categories (in years) | ||
| 11 to 14 | Ref | – |
| 15 to 17 | 0.54 | (0.16,1.83) |
| 18 to 21 | 0.67 | (0.21,2.26) |
| 22 to 38 | 0.30 | (0.08,1.08) |
| Gender | ||
| Male | Ref | – |
| Female | 0.77 | (0.28,2.11) |
| Clinical Characteristics | ||
| SNA (degree) | 0.96 | (0.84,1.11) |
| SNB (degree) | 0.96 | (0.84,1.11) |
| ANB (degree) | 0.90 | (0.61,1.34) |
| NA to Point A (mm) | 1.11 | (0.98,1.25) |
| NA to Pog (mm) | 1.07 | (0.98,1.15) |
| Wits (mm) | 0.98 | (0.85,1.14) |
| SNGo (degree)* | 1.10 | (1.02,1.18) |
| FMA (degree) | 1.00 | (0.94,1.07) |
| LAFH (mm)* | 0.90 | (0.82,0.99) |
| UISN (degree) | 1.04 | (0.98,1.11) |
| IMPA (degree) | 0.98 | (0.93,1.03) |
| ULS Plane (mm) | 1.04 | (0.85,1.27) |
| LLS Plane (mm) | 1.08 | (0.91,1.29) |
| ULE Plane (mm)* | 1.17 | (1.11,1.37) |
| LL to E plane (mm) | 1.10 | (0.95,1.28) |
| Overjet (mm)* | 1.84 | (1.33,2.54) |
| Overbite (mm) | 1.12 | (0.93,1.35) |
| Midline Lower (mm) | 1.48 | (0.86,2.56) |
| Midline Upper (mm) | 1.22 | (0.89,1.66) |
| Maxillary Crowding (mm)* | 2.26 | (1.47,3.45) |
| Mandibular Crowding (mm)* | 2.34 | (1.64,3.34) |
| NL Angle (degree)* | 0.95 | (0.91,0.99) |
a Reference category: Non-Extraction Treatment, *Significant at univariate (p<0.05).
According to Table 3, the odds of extraction treatment increase by 4.24 times (95%CI: 1.81, 9.95) as compared to non-extraction treatment as the mandibular crowding increases by 1mm adjusting for maxillary crowding and overjet. Similarly, the odds of extraction treatment increase by 9.25 times (95%CI: 2.20, 38.93) as compared to non-extraction treatment as the maxillary crowding increases by 1mm adjusting for mandibular crowding and overjet. Moreover, the odds of extraction treatment increase by 4.32 times (95%CI: 1.43, 13.05) as compared to non-extraction treatment as the overjet increases by 1mm adjusting for maxillary and mandibular crowding.
Table 3: Binary logistic regression analysis to study the orthodontic factors associated with extraction/non-extraction treatment groups.
| Extraction Treatment a | ||
| Independent Variables | Unadjusted OR (95% CI) b | Adjusted OR (95% CI) c |
| Mandibular Crowding ǂ (mm) | 2.34 (1.64, 3.34) | 4.24 (1.81, 9.95) |
| Maxillary Crowding ǂ(mm) | 2.26 (1.47, 3.45) | 9.25 (2.20, 38.93) |
| Overjet ǂ(mm) | 1.84 (1.33, 2.54) | 4.32 (1.43, 13.05) |
| SNGo (Degrees) | 1.10 (1.02, 1.18) | N. S |
| NL Angle (Degrees) | 0.95 (0.91, 0.99) | N. S |
| LAFH (mm) | 0.90 (0.82, 0.99) | N. S |
| ULE plane (mm) | 1.17 (1.00, 1.37) | N. S |
a Reference category: Non-Extraction Treatment b Univariate Binary Logistic Regression c Multivariable Binary Logistic Regression ǂ Significant at univariate and multivariable stage (p<0.05) N.S: Not significant at multivariable stage (p>0.05).
The findings of this research indicate that the decision-making in formulating treatment plans was significantly influenced by the degree of crowding in both arches, the incisal overjet, and the nasolabial angle. Hence, the study-cast analysis (including a space-analysis) and the cephalometric analysis significantly affect the clinical decisions in favor or against extractions.
Dental crowding has been amongst the top reasons for the extraction of teeth to align arches. Amongst the early orthodontists of the 20th century, Lundström was the first to declare, with much evidence, that there were much greater chances of treatments relapsing in crowded teeth that were aligned9. In more recent times, the notion that a certain degree of crowding necessitates dental extractions for stability in treatment outcomes is still endorsed with varying concerns largely dominated by the old paradigm of Angle which supported non-extraction treatments10,11. Guirro et al. studied the stability of the treatment outcome post-retention in Class I and II patients who were treated under extraction and non-extraction plans. Although they were unable to find any significant differences in the variables between the two groups, Class I cases exhibited more maxillary anterior dental crowding in late post-treatment stages in the group treated without extractions as compared to the one with extraction.
Another factor influencing the decisions to extract or not is the amount of overjet. The normal overjet is 2-4mm12. A significant difference of overjet with extractions seems to have been evident in several studies in the past few decades. Katsaros et al. in 1996 studied the differences in treatment-outcome of their Class I patients who were treated with and without extraction13.
The incisal proclination and protrusion were significantly greater in the patients treated under non-extraction plans. In more recent studies, the results concur with the findings of Ali et al. who studied factors affecting treatment decisions in their patients and stated that excessive overjet in Class I patients was corrected by extracting the first premolars and followed by retracting the anterior teeth14. Similar is the case with Kouli et al. who studied the effects of extraction and non-extraction treatment plans on Class I and Class II Subjects. They found a significant difference in the position of incisors being more forward and proclined in their Class I, non-extraction patients, amongst other differences15. Cotrin et al. compared relapse of overjet, overbite, and anterior crowding between extraction and non-extraction patients, and amongst their findings was a significant relapse of overjet in the non-extraction cases of Class I and II malocclusion16.
The third significant variable to direct the decisions is the nasolabial angle- “the angle formed between tangent to columella and tangent to upper lip”17. Extractions are normally prioritized for cases where the angle is acute and avoided when the angle is more obtuse. The ideal angle is 90-120°18-20. With age, the nasolabial angle becomes more obtuse and a short arch may lead to an even greater increase in the angle and hence a more aged appearance. Verma et al. studied the soft tissue profile differences in non-extraction and extraction cases of Class I malocclusion. Change of nasolabial angle was amongst the features which showed a significant difference between both the treatment groups with the angle showing an increase in the group which was treated with extraction21. Yashwant et al. evaluated changes in the soft tissue in the treatment of Class I patients between the two groups as well and found and concluded that nasolabial angle becomes more obtuse in cases that undergo extraction19. Further, in a meta-analysis by Almurtadha et al., it was assessed that nasolabial increases significantly in extraction cases compared to non-extraction ones22. Hence to base nasolabial angle as a guide to dictate the treatment decisions is plausible23. The current study is based on treatment decisions taken at a single center where cases are supervised by two trained orthodontists. This could create a bias in terms of the approach. Studies on the influencing factors could be spanned over multiple centers instead of one to reduce it. Future studies should be based in multiple centers and spanned across many areas of the region to understand psycho-social differences in treatment priorities throughout the region and aid to a global understanding of the various factors such as sense of dental esthetics, treatment priorities and variables that influence them.
The level of crowding in both the dental arches, the incisal overjet and the nasolabial angle are the variables that aid in the clinical decision-making for Class I malocclusion patients in terms of choosing an extraction or non-extraction plan. A higher degree of crowding, a greatly increased overjet and an acute nasolabial angle make orthodontists more inclined towards extractions for a harmonious and balanced occlusion and face profile of the patient.
The authors would like to acknowledge Dr. Ammar Ali Mohammad for his help in the statistical analysis and members of the Department of Orthodontics in their contribution to the data collection process.
The authors declare no conflict of interest.
Request for waiver of the Ethics Review Committee was put forward to the committee of Ziauddin University for the process as there was no patient contact, no new tests were done and patient confidentiality was maintained. The request was accepted and waiver No. 2951220HMOM was granted by the committee.
Covered under the waiver obtained by Ziauddin University as the waiver for this research was already obtained. All treatments commence with obtaining consent for using data for research purposes maintaining patient confidentiality.
HM collected and analyzed the data and was a major contributor in writing the manuscript. SM conceived the research idea, analyzed the data and was a major contributor in writing the manuscript. AK was a contributor in writing the manuscript.
- Mahmood TM, Qadir CA. Persuading factors for tooth extraction decision in treatment of class I malocclusion among orthodontists in Sulaimani city. J Dent Med Sci. 2015;14(8):20-28. doi: 10.9790/0853-14882028
- Proffitt WR, Fields Jr HW, Sarver DM. Contemporary Orthodontics. St Louis, MO: Mosby Elsevier; 2007. 50p.
- Konstantonis D. The impact of extraction vs nonextraction treatment on soft tissue changes in Class I borderline malocclusions. Angle Orthod. 2012;82(2):209-217. doi: 10.2319/051911-339.1
- Baumrind S, Korn EL, Boyd RL, Maxwell R. The decision to extract: part II. Analysis of clinicians’ stated reasons for extraction. Am J Orthod Dentofacial Orthop. 1996;109(4):393-402. doi: 10.1016/S0889-5406(96)70121-X
- Baumrind S, Korn EL, Boyd RL, Maxwell R. The decision to extract: part 1—interclinician agreement. Am J Orthod Dentofacial Orthop. 1996;109(3):297-309. doi: 10.1016/S0889-5406(96)70153-1
- Ruellas AC, Ruellas RM, Romano FL, Pithon MM, Santos RL. Tooth extraction in orthodontics: an evaluation of diagnostic elements. Dental Press J Orthod. 2010;15:134-157. doi: 10.1590/S2176-94512010000300017
- Tweed CH. Indications for the extraction of teeth in orthodontic procedure. Am J Orthod Oral Surg. 1944;30(8):405-428. doi: 1016/S0096-6347(44)90038-4
- Konstantonis D, Anthopoulou C, Makou M. Extraction decision and identification of treatment predictors in Class I malocclusions. Prog Orthod. 2013;14(1):1-8. doi: 10.1186/2196-1042-14-47
- Lundström AF. Malocclusion of the teeth regarded as a problem in connection with the apical base. Int J Orthod Oral Surg Radiograph. 1925;11(12):1109-1133. doi: 10.1016/S0099-6963(25)80052-8
- Peck S. Extractions, retention and stability: the search for orthodontic truth. Eur J Orthod. 2017;39(2):109-115.
- Angle EH. Treatment of Malocclusion of the Teeth: Angle’s System. Greatly Enl. and Entirely Rewritten, with Six Hundred and Forty-One Illustrations. SS White dental manufacturing Company; 1907. pp.393-402.
- Kinaan BK. Overjet and overbite distribution and correlation: a comparative epidemiological English-Iraqi study. Br J Orthod. 1986;13(2):79-86. doi: 10.1179/bjo.13.2.79
- Katsaros C, Ripplinger B, Högel A, Berg R. The influence of extraction versus non-extraction orthodontic treatment on the soft tissue profile. J Orofac Orthop. 1996;57(6):354-365. doi: 10.1007/bf02215673
- Ali B, Shaikh A, Fida M. Factors affecting treatment decisions for Class I malocclusions. Am J Orthod Dentofacial Orthop. 2018;154(2):234-237. doi: 10.1016/j.ajodo.2017.11.035
- Kouli A, Papagiannis A, Konstantoni N, Halazonetis DJ, Konstantonis D. A geometric morphometric evaluation of hard and soft tissue profile changes in borderline extraction versus non-extraction patients. Eur J Orthod. 2019;41(3):264-272. doi: 10.1093/ejo/cjy056
- Cotrin P, Freitas KM, Freitas MR, Valarelli FP, Cançado RH, Janson G. Evaluation of the influence of mandibular third molars on mandibular anterior crowding relapse. Acta Odontol Scand. 2020;78(4):297-302. doi: 10.1080/00016357.2019.1703142
- Setiawan SC, Widayati R, Sumardi S. Correlation in changes in the upper and lower incisor inclinations toward the nasolabial angle and mentolabial angle in non-extraction Class I malocclusion orthodontic treatment. J Phys Conf Ser. 2018;1073(6):1-6. doi :10.1088/1742-6596/1073/6/062002
- Celikoyar MM, Pérez MF, Akbaş MI, Topsakal O. Facial surface anthropometric features and measurements with an emphasis on rhinoplasty. Aesthet Surg J. 2022;42(2):133-148. doi: 10.1093/asj/sjab190
- Yashwant V A, Arumugam E. Comparative evaluation of soft tissue changes in Class I borderline patients treated with extraction and nonextraction modalities. Dental Press J Orthod. 2016;21:50-59. doi: 10.1590/2177-6709.21.4.050-059.oar
- Guirro WJ, Freitas KM, Janson G, de Freitas MR, Quaglio CL. Maxillary anterior alignment stability in Class I and Class II malocclusions treated with or without extraction. Angle Orthod. 2016;86(1):3-9. doi: 10.2319/112614-847.1
- Verma SL, Sharma VP, Tandon P, Singh GP, Sachan K. Comparison of esthetic outcome after extraction or non-extraction orthodontic treatment in class II division 1 malocclusion patients. Contemp Clin Dent. 2013; 4(2): 206-212. doi: 10.4103/0976-237X.114886
- Almurtadha RH, Alhammadi MS, Fayed MM, Abou-El-Ezz A, Halboub E. Changes in soft tissue profile after orthodontic treatment with and without extraction: A systematic review and meta-analysis. J Evid Based Dent Pract. 2018;18(3):193-202. doi: 10.1016/j.jebdp.2017.09.002
- Dardengo CD, Fernandes LQ, Capelli Júnior J. Frequency of orthodontic extraction. Dental Press J Orthod. 2016;21:54-59. doi: 10.1590/2177-6709.21.1.054-059.oar
This is an open-access article distributed under the terms of the CreativeCommons Attribution License (CC BY) 4.0 https://creativecommons.org/licenses/by/4.0/