By Fariya Usmani1, Syed Asif Ali1, Anum Naz2, Farhana3, Shahzaf Masood4, Huma Salahuddin5
AFFLIATIONS:
- Sir Syed Medical College, Karachi, Pakistan.
- Abbasi Shaheed Hospital, Karachi, Pakistan.
- Tibri Medical College, Karachi, Pakistan.
- Aga Khan University, Karachi, Pakistan.
- Department of Physiology, Ziauddin University, Karachi, Pakistan.
DOI: https://doi.org/10.36283/PJMD11-2/004
How to cite: Usmani F, Ali SA, Naz A, Farhana, Masood S, Salahuddin H. Comparative Effectiveness of Endoloop, Instrumental Tie and Ligaclip in Laparoscopy Appendectomy. Pak J Med Dent. 2022;11(2): 15-21. doi: 10.36283/PJMD11-2/004
Background: Appendectomy is the most commonly performed surgical procedure for patients. To examine the safety, complications, and cost-effectiveness of the instrumental tie, ligaclip and endoloop procedures have been used for the closure of the appendix stump. The objective of this study was to analyze the clinical outcomes, as well as to compare the effectiveness of the endoloop, instrumental tie, and ligaclip in laparoscopic appendectomy procedures.
Methods: The Sir Syed Medical College Hospital, Karachi was the center of this Randomized Control Study, from June 2020 to December 2020. Acute appendicitis patients (n=120) having age 7-85 years were categorized into three groups: A, B, and C. Ligaclips were applied to those in Group A, Instrumental Tie to Group B, and Endolope to Group C patients. Each group consisted of 40 participants. The Kolmogorov Smirnov test was used to determine the variables for normal distribution. The Chi-square test was used to measure the association between the duration of surgery and hospital stay.
Results: The statistical significance (p<0.05) of the relationship between the length of hospital stay and the duration of surgery had been established. The ligaclip demonstrates the shortest hospital stay of 2-3 days and the shortest operation time of 50-60 minutes, whereas the instrumental tie displayed the longest operation time of 72-75 minutes and the longest hospital stay of 4-5 days.
Conclusion: Ligaclip application of the appendiceal base showed statistically significant outcomes (p=0.00) regarding technical comfort, cost-effectiveness and operating time compared to endoloop and surgical tie applications.
Keywords: Ligaclip; Instrumental Tie; Endoloop; Laparoscopy Appendectomy.
Laparoscopic appendectomy, the most advanced method is less invasive and mostly preferred nowadays. There are various techniques; however, the surgeons are comparing the outcomes and effectiveness of instrumental tie, ligaclip and endoloop because these are more frequently used techniques in various tertiary hospital setups. In this setup, clinicians have witnessed the advantages and disadvantages of all these techniques1-3. In contrast with open medical procedure, laparoscopy has various benefits, including diminished postoperative agony, a more limited clinic stays, a speedier recuperation, and a diminished pace of wound disease. Even though laparoscopy relates to longer activity periods and more noteworthy activity costs, it is more useful and practical than opening a medical procedure for complexing an infected appendix when performed by qualified specialists. In any case, it is the best option for careful treatment and is shown especially in stout patients, old individuals, and those with critical comorbidities4,5.
Various investigations have been directed on the attached stump conclusion because of the assortment of accessible strategies: endoligature (counting performed stitch circles (endo-circles) and intracorporeal hitch tying stitches), bipolar coagulation, endoscopic straight cutting staplers, radiofrequency, ultrasonic vibrations, metal clasps or polymer cuts5,6. While figuring out which way to deal with the use, two basic elements should be thought of patient wellbeing and monetary expense. The previous alludes with the impacts of delayed sedation because of expanded usable time, iatrogenic injury, and reoperations for the deficient conclusion (e.g., stapler breakdown, circle disappointment, cut dislodgement), while the last refers to equipment costs per mediation and the expenses of longer methods (essentially decreased time for different tasks), delayed medical clinic stay, and cost of artful disease. Although, different examinations have been distributed contrasting the expenses and clinical results of these methodologies, this one is significant because it investigates four significant techniques for affixed stump conclusion in a randomized clinical four-arm preliminary5,7-9.
Endoligatures of a few assortments can be utilized to close the attached stump, including an endoloop, an intracorporeal tie, or a Roeder circle. The sort chosen is controlled by the specialist’s craving. Concerning the utilization of a solitary ligature versus two ligatures, contemplates discovered no genuinely huge distinction in the rate of postoperative confusions between the two choices; as it may be that the proof given by these investigations was of bad quality, as none of them incorporated into a randomized preliminary. Delibegovi and Mehmedovic utilized a solitary Vicryl circle ligature at the base and another at the distal end, which is then taken out using the appendix6,9,10.
There was a critical contrast in regards to careful time and base conclusion time in the favor of liga cuts (LIGACLIP Multi-Patient Clip Appliers are planned with grooves within jaw surfaces of the applier to increment in-jaw cut security). As mentioned earlier, all techniques have some advantages and disadvantages with ligaclips we have seen less number of complications and lesser hospital stay postoperatively with better patient comfort and satisfaction however; some studies reported in the favor of endoloop compared to other techniques11,12. Therefore, the objective of this study was to analyze the clinical outcomes, as well as to compare the effectiveness of the procedures like endoloop, instrumental tie, and ligaclip in laparoscopic appendectomy.
The simple randomized sampling was used in the study from June 2020 to December 2020. The Sir Syed Medical College Hospital, Karachi was the center of this Study. Acute appendicitis patients (n=120) were categorized into three groups: A, B, and C (n=40 each). The ethics approval was obtained from the Sir Syed Medical College and Hospital. The inclusion criteria involved both genders with ASA1/ASA2 and interval appendectomy. Age criteria were 7 to 85 years with all lap appendectomies. However, exclusion criteria involved peritonitis, appendicular abscess, patient refusal to laparoscopy procedure, lap converted to open, postoperative risk factors (ASA 3 and 4) and cecal/ appendiceal mass.
The demographic data of patients (age, gender, BMI (body mass index) were acquired from their medical records after taking informed consent. The duration of the procedure, the use of drains, and the length of hospital stay were all recorded. Patients were contacted one week after surgery for a follow-up appointment. The study examined early (30 days) postoperative complications. Acute appendicitis patients are classified into three groups: A, B, and C. ligaclips were applied to group A, the instrumental tie was applied to group B, and endoloop was applied to group C. The outcomes were quantified using the surgical time for each procedure and the length of stay in the hospital.
All procedures were carried out under general anesthetic. The monitor was positioned to the right of the patient, while the surgical team, comprising the operating surgeon and camera assistant, stood to the left of the patient. Each patient received a Foley catheter, which was withdrawn after the operation. The initial incision of the first port initiated the operational time.
Three ports were used to perform laparoscopic appendectomy. In patients with no prior abdominal surgery, a blind (Veress needle) or open (Hasson) approach was used to introduce an infraumbilical 10 mm port. The abdomen was explored using a 30o (degrees) laparoscope. The patients were placed in a slight trendelenburg position and then left decubitus. A second 10 mm port was introduced under direct vision from the left iliac fossa, and a third 5 mm hole was introduced above the pubis. The appendix was identified and deflammatory adhesions were removed. LigaSure™ was used to separate the mesoappendix (LigaSure™, Vessel Sealing System, Covidien, MA, USA).
A single non-absorbable polymeric Hem-o-lok® (Teleflex Medical; New York City, USA) clip or ENDOLOOP® Ligature was used to secure the appendiceal foundation (ETHICON; New Jersey, USA). LigaSure was used to separate the appendix right above the ligature. The appendix was extracted from the port in the left lower quadrant and placed either entirely within the port or in a surgical glove, depending on the appendix’s diameter. Following their removal, the diameters of the appendix specimens were reported. The entire abdomen was thoroughly inspected for intra-abdominal fluid and forcefully irrigated. Following bleeding control, the right lower quadrant was drained using a Jackson-Pratt drain and the port sites were closed. Operating time was halted after the conclusion of the last port site closure9.
At the time of anesthetic induction, all patients received a single dose of broad-spectrum intravenous antibiotic. Antibiotic administration postoperatively was determined by operational findings and postoperative sequelae. The descriptive statistics number (n), percentage, mean, and standard deviation were utilized to evaluate the data. The Kolmogorov Smirnov test was used to determine the variables’ normal distribution. The Chi-square test was used to measure the association between the duration of surgery and hospital stay. SPSS software was used to conduct the analyses and a significance level of p=0.05 with a 95% confidence interval was considered statistically significant.
The total 120 numbers of patients, with 40 of the patients to each surgeon. The study was designed by 3 surgeons and each surgeon had patients with all three techniques including: Ligaclip, Instrumental tie and Endoloop. The recorded BMI of males and females as shown below (Figure 1):
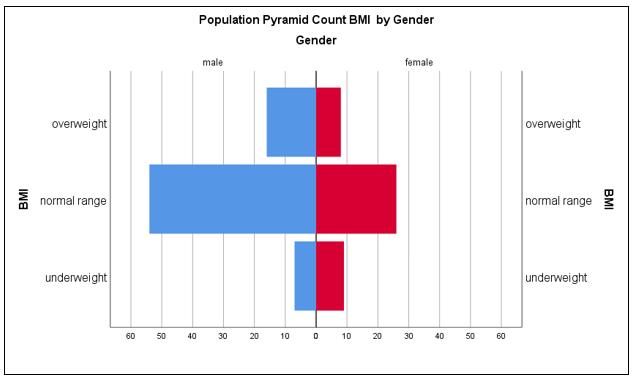
Figure 1: Correlation of gender with BMI of the patients.
The statistical measures of demographics of all the included participants were recorded and aligned as shown below in Table 1.
Table 1: Demographic characteristics of patients.
| Demographic Characteristics | Ligaclip
n (%) |
Endoloop
n (%) |
Instrumental Tie
n (%) |
p-Value |
| Age (years) (Mean ±SD) | 39.2 ±5.4SD | 42.5 ±5.9SD | 43.7 ±6.3SD | 0.452 |
| Gender (M: F) | 22:18 | 23:17 | 25:15 | 0.429 |
| BMI (Mean ±SD) | 26.3 ±4.5SD | 24.6 ±3.9SD | 27.8 ±4.4SD | 0.786 |
| Height (cm) (Mean ±SD) | 167 ±7.1SD | 164 ±6.7SD | 169 ±6.5SD | 0.341 |
| Weight (kg) (Mean ±SD) | 85.7 ±7.6SD | 78.3 ±6.8SD | 83.5 ±7.4SD | 0.442 |
| Hypertension (No. of Patients) | 14(35%) | 16(40%) | 17(42.5%) | 0.974 |
| Diabetes (No. of Patients) | 12(30%) | 14(35%) | 13(32.5%) | 0.546 |
| Smoking (No. of Patients) | 19 (47.5%) | 17 (42.5%) | 20(50%) | 0.528 |
The results reported that patients with group A had minimal hospital stay postoperatively with better patient compliance however, patients with group C had good patient satisfaction with slightly higher expenses comparatively than group A. On the other hand, group B showed poor outcomes compared to the other two groups. Group B had a longer operative time (Table 2).
Table 2: Surgical outcomes of the study.
| Variables | Ligaclip | Endoloop | Instrumental Tie | p-Value |
| Duration of Surgery(minutes) | 50-60 | 60-63 | 72-75 | <0.001 |
| Closing time of cystic duct and artery (minutes) (mean ±SD) | 6.3 ±1.2 | 7.8 ±1.5 | 8.2 ±1.6 | <0.001 |
| Length of Hospital Stay (days) | 2-3 | 3-4 | 4-5 | <0.001 |
| Drainage (n) | 33 | 30 | 32 | <0.561 |
| Complications (n) | 1 | 2 | 2 | <0.867 |
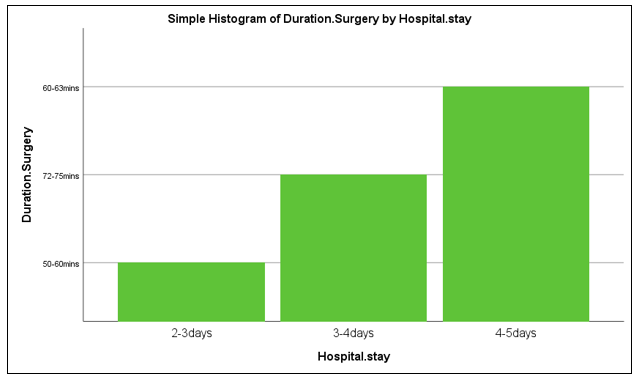
Figure 2: Duration of surgery and length of hospital stay of the patients.
The above graph depicted the least operation time and hospital stay with Group A (ligaclip) in, Group C (endoloop) with slightly greater operation time and highest hospital stay, while Group B (instrumental tie) had the highest operation time and 3-4 days of hospital stay. The p-value of Kolmogorov and Shapiro-Wilk was less than 0.05 hence; the research further proceeded for the parametric testing. Chi-Square was performed to assess the association between length of stay and duration of surgery. The demonstrated p-value suggested that there could be a significant association between the variables statistically (Table 3).
Table 3: Association between the length of hospital stay and duration of surgery.
| Chi-Square Tests | ||
| Pearson Chi-Square | Value | Asymptotic Significance (2-sided) |
| 240.000a | 0.000 | |
| Likelihood Ratio | 263.667 | 0.000 |
| Linear-by-Linear Association | 119.000 | 0.000 |
| N of Valid Cases | 120 | |
| a. 0 cells (0.0%) have an expected count less than 5. The minimum expected count is 13.33. | ||
The most exceptional strategy for a laparoscopic appendectomy is less intrusive. That implies its management without an enormous cut. Overall, from 1 to 3 little cuts are made with a long, slender cylinder called a laparoscope is placed into one of the cuts. It has a minuscule camcorder and careful devices. The specialist takes a gander at a TV screen to see inside patient’s mid-region and directs the devices13.
The reference section is eliminated through one of the entry points. These days, specialists have different strategies to close the foundation of the reference section considering numerous variables, which incorporates insignificant intricacies, better security and less medical clinic stay. A sufficient conclusion of the appendiceal stump is fundamental to limit intra-stomach and careful site contaminations. There are different methods for the conclusion of the base of the index while carrying out a laparoscopic appendectomy like endoloop, tying, clasps and staplers14.
In the current study, Endoloop Ligature, Instrumental tie and ligaclips were considerably observed based on their utilization in laparoscopic appendectomy. There was a huge distinction regarding to time management and base conclusion time of liga cuts. All strategies employ a few benefits and impediments identified with the actual material or the technique. Safety, application solace, unfamiliar body effects of the materials and working time, are the central subjects characterizing the assortment of the strategies. The ideal technique would be the quickest and most secure approach to close the foundation of the index related with no drawn-out entanglement15.
The surgeons had seen the ligaclips diminish time in the hospital setup and consider this as an economically valuable and easy option to broadly use endoloop and surgical tie. The incidence of complications post laparoscopic appendectomy with ligaclip was lesser than with the other two techniques. A study reported that endoloop can be securely selected and must be the chosen modality in assessing the stump, particularly for lower-level appendix infection but for complicated appendicitis, the results can vary16.
Delibegović and Mehmedovic previously investigated the tissue reactions of polymeric Hem-o-lok clips and endoloops in the gut using a rat model. The study’s findings indicated that both equipments had a satisfactory degree of reaction of foreign objects and that the polymeric clips had a little lower degree of tissue reaction than endo-loops2. Moreover, Hanssen et al. discovered that the usage of polymeric clips is safe and effective, with an emphasis on cost effectiveness8.
Hue et al. published another study in which they compared the endoloop ligature to a polymeric ligaclip in LA. The investigators discovered no considerable differentiation statistically in the feasibility and safety of the procedure between these two approaches17. Unfortunately, the time during the surgery, which was observed shorter in the investigation, was not analyzed in this research. The findings indicated that polymeric clip applications outperformed conventional clip applications in terms of technical comfort and operational time. Further clinical investigations, particularly on the long-standing security of this approach, are required to obtain a definitive ending17.
Laparoscopic appendectomy is becoming more common than open appendectomy because it offers benefits such as a shorter hospital stay, quicker healing, less pain, and a higher quality of life. This procedure’s most important stage is appendix stump closure. Although, some surgeons utilize solely coagulation devices to close stumps, most surgeons are still hesitant because complications such as an intra-abdominal abscess can occur because of stump leakage18.
In an open appendectomy, the stump can be simply fixed with a simple knot or purse-string suture in more difficult instances19. There are numerous ways for securing the stump in LA, including intra- or extracorporeal simple ties, endoloops, metal or polymeric clips, and endo-staplers. There have been studies comparing these procedures, though none have yet compared hand-made extracorporeal knotting with polymeric clips20.
Strzałka et al. with 307 laparoscopic appendectomy patients, compared metal clips, sutures, and endo-staplers, and found no statistical difference in complications between the three procedures11. Matyja et al. also assessed all three procedures, found no differences between them, stating that endoscopic staplers are more expensive, and should only be used if other methods fail to close the stump12.
One of the current study’s weaknesses is that both investigations are retrospective. Endoloops, on the other hand, are safe even in difficult instances, although they are very expensive21-23. The use of an endoloop may lengthen the procedure. Some experts found that the endoloop group took longer to operate, while Kazemier et al. discovered the opposite13. The surgeons feel that using an endostapler through a 15mm trocar increases the chance of a trocar site hernia, in addition to increasing the cost and surgery duration. When previous procedures fail to secure the appendix stump, an endostapler should be employed24,25.
Bali et al. examined endoloop and intracorporeal knotting and found no significant differences between groups other than operation time. When intracorporeal knotting was used, the average operation time increased by about 5.6 minutes (p=0.01)15. Kiudelis et al. compared intracorporeal knotting with invaginating suture with endoloop in a prospective analysis of 152 patients, finding that endoloop reduced surgery time (p>0.05) but increased the cost by around 80€ per patient. As a result, endoloop has the advantage of a shorter operation time but with a higher cost16.
The application comparison of Ligaclip to the appendiceal base to that of Endoloop and Surgical Tie, the results were statistically significant, while considering technological and comfort aspects along with cost-effectiveness and surgery time efficiency.
The authors would like to acknowledge hospital staff and doctors for their immense contribution. They are thankful to the ERC board of SSMC to provide the permission for carrying out the study in the hospital.
All authors declared no conflict of interest.
The ethics approval was obtained from the Sir Syed Medical College and Hospital.
Written consent was taken from all the patients included in the study.
FU helped in data collection procedures. SAA was the principal researcher, carried out the research procedures. AN assisted in statistics and HS helped in manuscript writing. F and SM assisted in data collection.
- Semm K. Endoscopic appendectomy. Endoscopy. 1983;15(02):59-64. doi: 10.1055/s-2007-1021466rt
- Delibegović S, Mehmedovic Z. The influence of the different forms of appendix base closure on patient outcome in laparoscopic appendectomy: a randomized trial. Surg Endosc. 2018;32(5):2295-2299. doi: 10.1007/s00464-017-5924-z
- Sahm M, Kube R, Schmidt S, Ritter C, Pross M, Lippert H. Current analysis of endoloops in appendiceal stump closure. Surg Endosc. 2011; 25(2):124-129. doi: 10.1007/s00464-010-1144-5
- Swiss Association of Laparoscopic and Thoracoscopic Surgery Study Group Beldi G guido. beldi@ insel. chVorburger SA, Bruegger LE, Kocher T, Inderbitzin D, Candinas D. Analysis of stapling versus endoloops in appendiceal stump closure. J Br Surg. 2006;93(11):1390-1393. doi: 10.1002/bjs.5474
- Ates M, Dirican A, Ince V, Ara C, Isik B, Yilmaz S. Comparison of intracorporeal knot-tying suture (polyglactin) and titanium endoclips in laparoscopic appendiceal stump closure: a prospective randomized study. Surg Laparosc Endosc Percutan Tech. 2012;22(3):226-231. doi: 10.1097/SLE.0b013e31824f25cd
- Rakić M, Jukić M, Pogorelić Z, Mrklić I, Kliček R, Družijanić N, et al. Analysis of endoloops and endostaples for closing the appendiceal stump during laparoscopic appendectomy. Surg Today. 2014;44(9):1716-1722.
- Gomes CA, Junior CS, de Peixoto RO, Netto JM, Gomes CC, Gomes FC. Appendiceal stump closure by metal endoclip in the management of complicated acute appendicitis. World J Emerg Surg. 2013;8(1):1-5. doi: 10.1186/1749-7922-8-35
- Hanssen A, Plotnikov S, Dubois R. Laparoscopic appendectomy using a polymetric clip to close the appendicular stump. J Soc Laparoendosc Surg. 2007; 11(1): 59-62. 2007;11(1):59-62.
- Kothari R, Somashekar U, Sharma D, Thakur DS, Kumar V. A simple and safe extracorporeal knotting technique. J Soc Laparoendosc Surg. 2012;16(2):280-282.doi: 10.4293/108680812X13427982376941
- Mayir B, Bilecik T, Ensari CO, Oruc MT. Laparoscopic appendectomy with hand-made loop. Wideochir Inne Tech Maloinwazyjne. 2014; 9(2): 152-156.doi: 10.5114/wiitm.2014.41624
- Strzałka M, Matyja M, Rembiasz K. Comparison of the results of laparoscopic appendectomies with application of different techniques for closure of the appendicular stump. World J Emerg Surg. 2016;11(1):1-6. doi: 10.1186/s13017-015-0060-3
- Matyja M, Strzałka M, Rembiasz K. Laparosocopic appendectomy, cost-effectiveness of three different techniques used to close the appendix stump. Polish J Surg. 2015;87:634-637. doi: 10.1515/pjs-2016-0015
- Kazemier G, Saad S, Bonjer HJ, Sauerland S. Securing the appendiceal stump in laparoscopic appendectomy: evidence for routine stapling? Surg Endosc. 2006;20(9):1473-1476. doi: 10.1007/s00464-005-0525-7
- Partecke LI, Kessler W, Patrzyk M, Heidecke CD, Bernstorff WV. Comparison among different closure methods of the appendicular stump in laparoscopic appendectomy. Surg Technol Int. 2011;21:85-91.
- Bali İ, Karateke F, Özyazıcı S, Kuvvetli A, Oruç C, Menekşe E, et al. Comparison of intracorporeal knotting and endoloop for stump closure in laparoscopic appendectomy. Ulus Travma Derg. 2015;21(6):446-449. doi: 10.5505/tjtes.2015.56798
- Kiudelis M, Ignatavicius P, Zviniene K, Grizas S. Analysis of intracorporeal knotting with invaginating suture versus endoloops in appendiceal stump closure. Wideochir Inne Tech Maloinwazyjne. 2013; 8(1): 69-73.doi: 10.5114/wiitm.2011.31535
- Hue CS, Kim JS, Kim KH, Nam SH, Kim KW. The usefulness and safety of Hem-o-lok clips for the closure of appendicular stump during laparoscopic appendectomy. J Korean Surg Soc. 2013;84(1):27-32. doi: 10.4174/jkss.2013.84.1.27
- Rickert A, Bönninghoff R, Post S, Walz M, Runkel N, Kienle P. Appendix stump closure with titanium clips in laparoscopic appendectomy. Langenbecks Arch Surg. 2012;397(2):327-331. doi: 10.1007/s00423-011-0869-5
- Akbiyik F, Senel E, Bayram-Kabacam G, Demirkan H, Atayurt H, Tiryaki T. A comparison of polymer clips and endoloop applications for securing the appendiceal stump during laparoscopic surgery in children. Surg Laparosc Endosc Percutan Tech. 2011;21(5):349-352.doi: 10.1097/SLE.0b013e31822d68ca
- Colak E, Kement M, Ozlem N, Mutlu T, Yildirim K, Gurer A, Aktimur R. A comparison of nonabsorbable polymeric clips and endoloop ligatures for the closure of the appendicular stump in laparoscopic appendectomy: a prospective, randomized study. Surg Laparosc Endosc Percutan Tech. 2013;23(3):255-258.doi: 10.1097/SLE.0b013e31828b8382
- Lucchi A, Berti P, Grassia M, Siani LM, Gabbianelli C, Garulli G. Laparoscopic appendectomy: Hem-o-lok versus Endoloop in stump closure. Updates Surg. 2017;69(1):61-65.10.1007/s13304-016-0413-9
- Wilson MS, Maniam P, Ibrahim A, Makaram N, Knight SR, Patil P. Polymeric clips are a quicker and cheaper alternative to endoscopic ligatures for securing the appendiceal stump during laparoscopic appendicectomy. Ann R Coll Surg Engl. 2018;100(6):454-458. doi: 10.1308/rcsann.2018.0036
- Parlakgumus A, Ezer A. Polymeric clips for stump closure in laparoscopic appendectomy. J Coll Physicians Surg Pak. 2017;27:660-662.
- Arer IM, Avci T, Yabanoglu H. Hand-made extracorporeal knotting versus hem-o-lok clip for stump closure in laparoscopic appendectomy. J Coll Physicians Surg Pak. 2019;29(12):1203-1206.
- Elmeligy HA, Abdalgaliel MM, Gomaa AM. Laparoscopic appendectomy with clipping versus intra-corporeal ligation for securing the appendiceal stump. Eur J Mol Clin Med. 2021;8(2):2539-2547.
This is an open-access article distributed under the terms of the CreativeCommons Attribution License (CC BY) 4.0 https://creativecommons.org/licenses/by/4.0/