By Arsia Hanif1, Sana Shahid2, Niaz Hussain Soomro3, Ummalqura Sarosh2, Sana Jawed1
AFFLIATIONS:
- Dow University of Health Sciences, Karachi, Pakistan.
- Civil Hospital, Karachi, Pakistan.
- Department of Thoracic Surgery, Ojha Institute of Chest Disease, Dow University of Health Sciences, Karachi, Pakistan.
An azygos lobe of a lung, a rare anomaly or anatomical variant of the lung formed during embryogenesis when the posterior cardinal vein deviates from its normal migration path. Clinically, azygos lobe can imitate various ailments. Most commonly, it is found incidentally and usually involved the right lung. ‘Azygos’ means ‘an unpaired structure’ in the Greek language. Discussed here, is a rare case of a 35-year-old patient who presented with symptoms of a lung hydatid cyst but was incidentally diagnosed with azygos lobe on the computed tomography scan. The imaging findings were confirmed intraoperatively during the excision of the ruptured hydatid cyst of the lung. It is crucial for physicians to know about this rare anatomical variant of the lung to avoid a misdiagnosis. It is even more important for thoracic surgeons to be aware of an azygos lobe of the lung so they can predict and avoid its associated complications during thoracic surgery.
Keywords: Azygos Vein; Lung; Hydatid Cyst; Thoracic Surgery.
An azygos lobe of the lung is a rare anatomical variant of the right lung which is found in only 0.4% of the individuals in clinical settings, i.e., on chest radiographs and in only 1% of the anatomical specimens1. It is formed during embryonic development when the thoracic portion of the azygos vein, instead of arching over the right lung’s apex, penetrates through the right lung’s upper lobe. This deviation creates an accessory fissure, called the azygos fissure, which delineates a portion of the lung, called the ‘azygos lobe’ 2. The following case describes an incidental finding of an azygos lobe and fissure in a patient who presented with clinical manifestation of a hydatid cyst.
A 35-year-old male presented to the outpatient department with complaints of right-sided chest pain for the past 6 months. The patient also complained of shortness of breath, productive cough, and hemoptysis for the past 3 months. He had a 10-pack-year history of smoking but had quitted smoking 5 years back. His right-sided chest pain started abruptly 6 months back, for which he received treatment from a local clinic, and he felt better. Around 3 months later, he again had another episode of sudden chest pain with shortness of breath, productive cough, and hemoptysis. According to the patient, he would cough approximately 2 cups of blood mixed with sputum, at least twice or thrice in a day. The patient had no fever, rash, or any other symptoms. He was admitted to the pulmonology unit, where he underwent investigations to rule out tuberculosis (TB). His TB investigation results came back negative, but he was diagnosed with a right-sided hydatid cyst of the lung. He was managed conservatively with albendazole 400 mg twice daily for 28 days. The patient had improved symptomatically until the current presentation.
During the current presentation, he presented with chest pain and dyspnea on rest. He also complained of cough with blood-streaked sputum. He was admitted with a working diagnosis of a ruptured hydatid cyst of the lung. Physical examination revealed decreased breath sounds in the right hemithorax. The patient had a positive Echinococcus antibody IgG assay. A contrast-enhanced computed tomography scan (CT) of the chest and upper abdomen revealed loss of right lung volume and a thin-walled cavitary lesion in the anterior segment of the right lung measuring 5.9×6.3×9.0 cm, with air-fluid levels and thin septae. Adjacent patchy consolidation was also appreciated. Right upper lobe showed a tree-in-bud appearance, i.e., centrilobular ground-glass nodules with impacted bronchioles. The right peri-bronchial region had an ill-defined soft tissue thickening which was seen encasing the right mainstream bronchus causing slight luminal narrowing. Few calcified granulomas were also seen in the anterior segment of the right lower lobe.The pre- and paratracheal lymph nodes measured 2.0×1.8 cm. Besides, the CT scan also incidentally revealed a rare finding of an azygos lobe and azygos fissure (Figure 1).
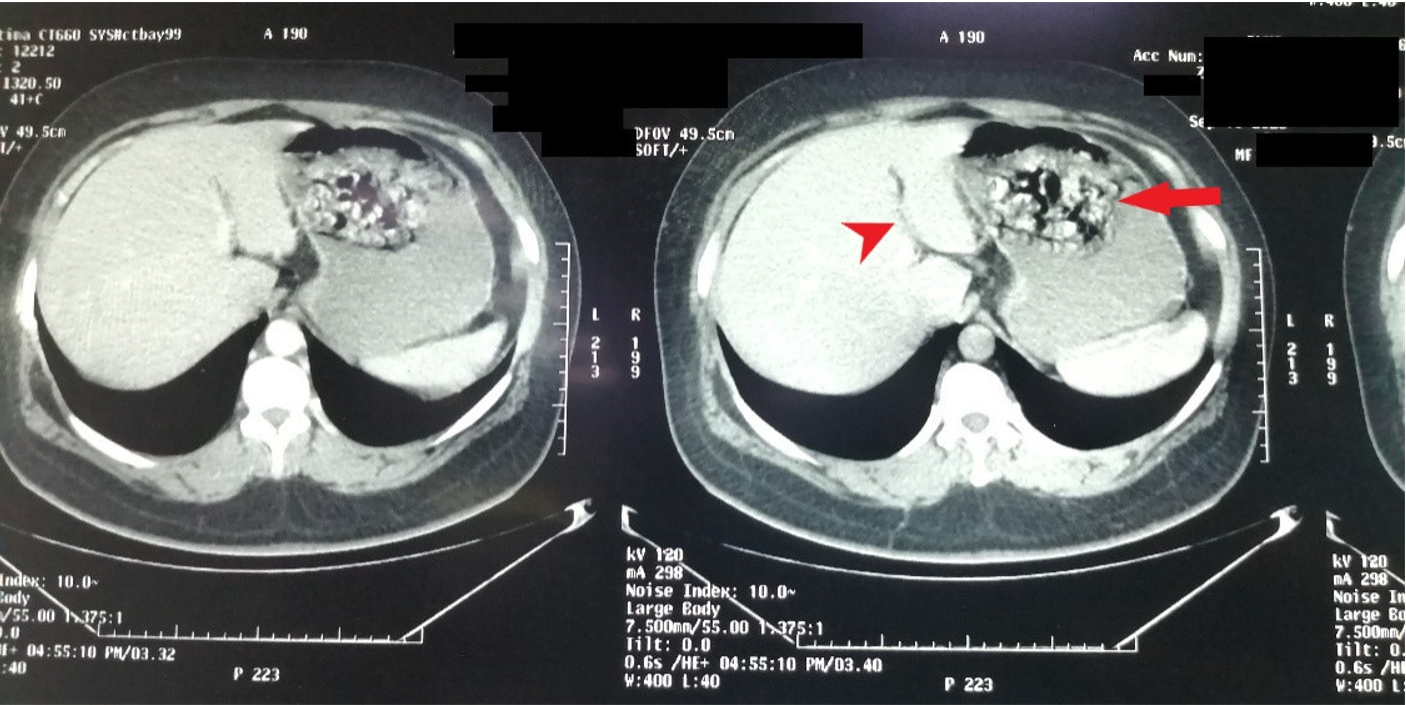
Figure 1: CT scan of the chest showing an azygos fissure and azygos lobe of the lung (arrowhead) and a ruptured hydatid cyst (arrow).
It was decided to perform right posterolateral thoracotomy. Intraoperatively, a large, ruptured cyst was found in the right lobe of the lung which was excised successfully (Figure 2a). Air leaks were identified and repaired. Two chest drains were placed and connected to the Pleur-evac® unit. Additionally, an azygos lobe was appreciated intraoperatively, concurring with the CT scan findings (Figure 2b). The postoperative course was unremarkable, and the patient was continued on albendazole. The histopathological report confirmed the Echinococcal hydatid cyst. The patient was discharged on the 10th postoperative day. At the 6-month follow-up, a well expanded right lung was seen on a chest X-ray.
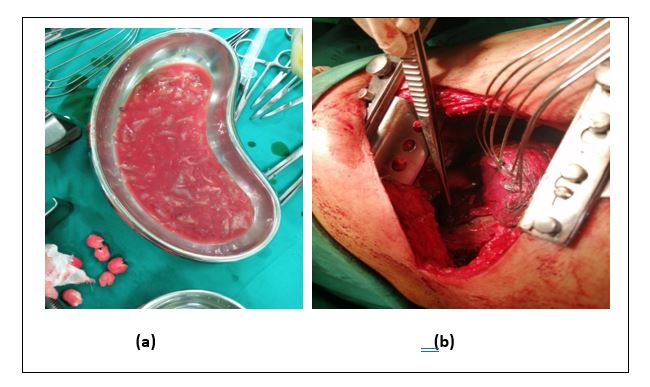
Figure 2a: Removed ruptured cyst; b: Forceps pointing to an azygos lobe of lung.
An azygos lobe of the lung is a rare anomaly of the lung, usually asymptomatic and found incidentally on imaging studies. It is usually seen in the apicomedial part of the right lung3. In some individuals with an azygos lobe, an accessory fissure called the azygos fissure is also seen. It forms when the thoracic portion of the azygos vein penetrates the lung while dragging both the layers of pleura with it4, and it appears as a fine, convex, opaque line running across the apical part of the right lung obliquely5. The fissure, thus, delineates a segment of the lung’s lobe, which is called the azygous lobe, and the presence of the fissure on imaging helps in identifying the azygos lobe. The azygos lobe has an upper triangular-shaped part, known as “trigonum parietale”, and a lower portion resembling a teardrop. The former contains areolar tissue while the latter contains the azygos vein. Since the azygous lobe, does not have its specific bronchial supply, it is not a true lobe. In fact, the airways for the azygous lobe come from the posterior or apical segments of the upper lobe of the right lung6.
According to the migratory course of the vein, the then formed azygos fissure can either be classified as type A, type B, or type C5. It is classified as type A fissure when it is somewhat horizontal; type B when the fissure vertically divides the apex into two halves, and type C is when it starts from the mediastinal side of the lung and vertically passes through, delineating a small portion of the upper lobe. This patient had an azygos fissure, which was consistent with type A.
Although individuals with an azygos lobe and fissure are usually asymptomatic and are diagnosed incidentally, some patients may present with symptoms too. For instance, patients may present with recurrent hemoptysis due to compression of the right upper lobe by the azygos lobe. In addition, a deep azygos fissure may lead to bronchiectasis or atelectasis by compressing the underlying bronchus7. In addition, if the azygos vein, which resulted in the formation of an azygos lobe, develops an aneurysm, the affected individual may complain of chest tightness or a pressure-like feeling within the chest.
Conversely, an azygos lobe may play a role in confining the pathology arising within it. In addition, the pleural folds may act as a barrier, protecting the azygos lobe from the pathology of the rest of the lung. For example, pulmonary tuberculosis affecting the entire lung may not spread to the azygos lobe. Denega et al. reported that malignancy of the azygos lobe remains confined to the azygos lobe3. This was further supported by another study confirming negative mediastinal lymph nodes with squamous cell carcinoma of the azygos lobe8. Fukuhara et al. reported a case of adenocarcinoma of the azygos lobe of the lung, which remained confined with the boundaries of the azygos lobe without any metastasis to the regional lymph nodes8. Additionally, azygos lobe has been seen playing a role in protecting the lung against spontaneous pneumothorax9 by protecting against the development of bullae and blebs in the apical region of the lung, which are common findings in patients with spontaneous pneumothorax.
Although clinically, an azygos lobe is accepted to be a normal variant10 or a benign anomalythat has no health consequences, it has a significant impact on the anatomy of the mediastinum. For instance, the presence of azygos lobe may alter the shape of the superior vena cava and may even displace it slightly. Moreover, radiologically it may mimic other pathologies. On imaging, it may appear as bullae, abscesses, paratracheal opacity, enlarged thymus, a substernal goitre, or a lung mass5. Therefore, if plain radiographs are inconclusive, computed tomography scans should be done to delineate the anatomy of the lobe, identify the normal position of the azygos vein, and identify the underlying pathology, if present. Moreover, during thoracoscopic procedures, an azygos fissure may increase the risk of bleeding and damage to the phrenic nerve if it is coursing within the azygous fissure; and an azygoslobe may obstruct the view10. Some have reported difficulty in reflecting the pleura during surgery due to the presence of azygos fissure, while others have reported a partially hindered view during sympathectomy6.
A rare anatomical variant azygos lobe develops usually in the right lung when the azygos vein deviates from its normal migratory path. Although, many individuals may not be even diagnosed in their lifetime, as it usually remains asymptomatic. It is important to be aware of this rare variant as radiologically it may disguise as other lung pathologies and may increase the surgical challenges, especially for a thoracic surgeon. Therefore, knowing the significance of azygos lobe, fissure and their clinical relevance can avoid premature diagnosis, undue investigations/interventions, and surgical complications.
The authors would like to acknowledge the Ojha Institute of Chest Diseases of Dow University of Health Sciences for facilitating the study.
The authors declare no conflict of interest.
Verbal and written consent was taken from the patient.
AH is the corresponding author, interpreted the data, designed, and submitted the case. SS and NHS performed clinical examinations and reviewed the work. SJ and US assisted in the critical revision of the case. No disclosure to be made. All authors read and approved the final manuscript.
- Felson B. The azygos lobe: its variation in health and disease. Semin Roentgenol. 1989;24(1):56-66.
- Tran CT, Miao KH, Lui F. Anatomy, Thorax, Lung Azygos Lobe. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2020. Available from: https://europepmc.org/article/nbk/nbk518977#_article-18070_s1_
- Denega T, Alkul S, Islam E, Alalawi R. Recurrent hemoptysis – a complication associated with an azygos lobe. Southwest Respir Crit Care Chron. 2015;3(11):44-74.
- Kotov G, Dimitrova I, Iliev A, Groudeva V. A rare case of an azygos lobe in the right lung of a 40-year-old male. Cureus. 2018;10(6):1-5.
- Stawicki S, Wall J. The azygos lobe. Int J Acad Med. 2017;3(3):189-190.
- Butler P, Mitchell AW, Ellis H, editors. Applied radiological anatomy. Cambridge University Press; 1999. 6p.
- Ndiaye A, Ndiaye N, Ndiaye A, Diop M, Ndoye J, Dia A. The azygos lobe: an unusual anatomical observation with pathological and surgical implications. Anat Sci Int. 2012;87(3):174-178.
- Fukuhara S, Montgomery M, Reyes A. Robot-assisted azygos lobectomy for adenocarcinoma arising in an azygos lobe. Interact Cardiovasc Thorac Surg. 2013;16(5):715-717.
- Çimen M, Erdil H, Karatepe T. A cadaver with azygos lobe and its clinical significance. Anat Sci Int. 2005;80(4):235-237.
- Moon SW, Yoon JS, Jo KH, Wang YP, Park HJ. Thoracoscopic sympathetic clamping in a patient with an azygos fissure. Surg Laparosc Endosc Percutan Tech. 2005;15(2):110-111.
This is an open-access article distributed under the terms of the CreativeCommons Attribution License (CC BY) 4.0 https://creativecommons.org/licenses/by/4.0/