By Waqar Ahmed Memon1, Salman El Khalid2, Imran Sharif 2, Sherjeel Saulat3, Ali Haider4, Asadullah5, Sana Tariq3
AFFILIATIONS:
- Department of Urology, Liaquat University of Medical and Health Sciences.
- Department of Urology, the Kidney Centre Post Graduate Training Institute.
- Department of Urology, Tabba Kidney Institute Post Graduate, Training and Research Center.
- Department of Surgery, Hamdard University Hospital, 5Department of Urology, Balochistan Institute of Nephrology Urology Quetta (BINUQ), Quetta, Balochistan, Pakistan.
ABSTRACT
Background: Double J stent is used to prevent complications after extra corporeal shockwave lithotripsy (ESWL) like ureteric obstruction. Extent the ureteral stent affects stone fragments passage in patients, with renal stone, who had shock wave lithotripsy. Therefore, the objective of the study was to evaluate the efficacy of Double J stent on stone clearance after extra corporeal shockwave lithotripsy.
Methods: A total of 194 patients with pelvic renal stones were treated with extra corporeal shockwave Lithotripsy, divided into two groups: Group 1 represents n= 97, 50%, patients with double-J (DJ) stent while, Group 2 n= 97, 50%, patients without DJ stent. These patients were further subdivided into two more groups as per stone burden: Group A n=184, 94.4% hold the stone size of ≤ 1.0 cm – 2.0 cm and Group B, n=11, 5.6% consisted of 2.1 cm – 3.0 cm stone size. The effect of DJ stent on stone passage was evaluated by statistical analysis included Chi-squared, Mann-Whitney U test, Cross-Tabulation and p-value=0.05 was considered statistically significant.
Results: Among 194 patients, the male: female ratio was 136(69.7%):55 (30.0%) with a mean age of 42.77±14.24. Single and multiple stones were present in 133(68.2%) and 62(31.8%) respectively. In cross-tab analysis stone clearance rates were 83(42.7%) with DJ stenting while 14 (7.2%) stones were pending, similarly, 87(44.8%) were stone free without DJ stenting and 10(5.1%) were pending. Large stones were reportedly more prone to complications such as hematuria and loin pain (p=0.074).
Conclusion: Stone free rate is significantly higher in the non-stented group than in stented with pelvic renal stone.
Keywords: Renal Stones; DJ Stents; Lithotripsy, DJ Stent Complications.
One of the most attributed pathological conditions in medicines is urinary tract stone. Especially in low-income countries such as Pakistan, India, Bangladesh and Nepal, the incidence rate of kidney stone disease is remarkably higher than in high-income economies of the world. Not only contributing to a higher risk of renal failure but also enormously affecting socio-economic status too1. The chances of an individual getting renal stone in a lifetime are 12% according to the prevalence rates, some stones are called silent stones, and may remain in the renal system, for weeks to years without causing any problem, and these stones are more dangerous than symptomatic. In order to find stones in the early stages when the size of the stone is small and clinically significant to remove without invasive procedures is vital. To eradicate renal stones in the pediatric and adult population there are so many procedures being implied in urology from the last two decades, including percutaneous lithotripsy (PCNL), mini percutaneous lithotripsy (PCNL), micro percutaneous lithotripsy (PCNL), and extracorporeal shockwave lithotripsy (ESWL), still the most preferred treatment for ureteral and kidney stones are debatable. Ureteral stents are favorite first line treatment options of urologists for decades2-5. Ureteral stent also commonly used to help stone passage before and after invasive or non-invasive procedures6,7.
Studies supported the role of Double J stent to facilitate stone passage by dilating the ureter; JJ stent reportedly decreases the chances of renal colic and different complications such as Hematuria, lower urinary tract symptoms (LUTs) and urinary tract infections (UTIs). Double J stent placement prevents (i) ureteric obstruction (post extracorporeal shock wave lithotripsy (ESWL) (ii) internal renal drainage (post-stone removal) (iii) ureteric splinting (post-ureteric reconstruction)8-10. In 1980, the introduction of ESWL reformed the treatment options for urolithiasis6.
Extracorporeal shockwave lithotripsy (ESWL) holds the position of the most preferred treatment method in many ureteric and kidney stone diseases. The success rate is strictly tangled with some contributing factors such as the location of renal stone, size, composition, and distance of skin and stone. Particularly, clinical indications for ESWL are represented by <1 cm stone in the kidney or proximal-distal ureter. After the evaluation of these factors, it helps in the complete fragmentation of urinary stones and hence the technical success of ESWL, the occurrence of complications due to the traumatic effect of the shock wave on body tissues and in particular on urinary tract has to be considered10. Double J stent is helpful in urolithiasis treatments, also promoting ureteral healing and help in stone passage after breakage, but apart from their advantages when administered Double J stents may cause stent-related symptoms (SRSs) regardless of the duration. The most common symptoms related to double J stent along with LUTS are frequency, urgency, and dysuria with 60% and 40% respectively, hematuria with 18.1% and flank pain 25.3% ultimately reducing a patient’s quality of life and compromise their comfort11. DJ stents placement after ESWL to eliminate renal calculi is controversial.
According to the old rationale, “the use of ureteral stents reduces complications after ESWL and contributes to successful stone passage. However, some reports noted complications that are attributed to indwelling ureteral stents and concluded that ureteral stents do not reduce post-shockwave lithotripsy (SWL) complications and they are clearly associated with morbidity and do not improve stone passage markedly”11. Double J stenting is not helpful in the stone passage or complications reduction related to ESWL, concluding that stenting is almost unnecessary in extracorporeal shockwave lithotripsy in ≤ 2.0 cm of stones9. Another RCT study results have shown that Double J stent placement has no positive effect on stone passage or reduction of complications after ESWL12.
Studies also reported many serious complications such as vesicoureteral reflux and partial obstruction13 except for LUTs and other complications reported after DJ insertion. The epidemiological result shows the registration of 1-3 per thousand patients of urinary calculi, making them 15-24% 14. In the last few decades ESWL is not been in use as much previously although the efficacy is been proven in many studies the controversy regarding the effect of Double J stent after ESWL on stone clearance rate needs more evaluation. The purpose of this study is to understand the positive and negative effects and outcomes of DJ stent usage after ESWL to estimate the success rate contribution provided by DJ stents in non-invasive urological procedures. This study aimed to get profound knowledge on contributing factors involved in stone-free rates and stone passage after ESWL, improve stone clearance rates, and reduce obstructions caused after lithotripsy.
This is a retrospective cross-sectional study conducted on 194 patients who were enrolled and treated with extracorporeal shockwave lithotripsy in the urology Department of the Kidney Centre, Postgraduate Training Institute Karachi, Pakistan, from 2018 January to 2019 January. Patients were divided into two groups I, II and A, B according to DJ stent embedding and the difference in stone sizes respectively. The patients (n=97) were enrolled with DJ stent while n=97 patients were without DJ stenting. The patients were then subdivided into two groups as per stone size, group A (n=184, 94.4%) represents the stone burden of ≤ 1.0 cm – 2.0 cm while Group B (n=11, 5.6%) consists stone size of 2.1 cm – 3.0 cm.
The inclusion criterion for the study is of patients with renal stones of ≤ 1.0 cm –3.0 cm, only pelvic stones were included without any history of open renal surgery or severe co-morbidities, the imaging technique used to confirm the location of stones was kidneys, ureter and bladder (KUB) ultrasound. While renal stones of >1.0 cm or <3.0 cm, stone located in calyxes or ureter (proximal, mid or distal), polar stones, previous history of open renal surgery, impaired kidney function test and coexisting anatomical abnormalities, (calyceal diverticulum, renal ectopia, horseshoe kidney) were excluded.
Success in terms of stone-free rate (SFR) after ESWL was documented along with the total number of sessions required for complete stone clearance noted along with energy, number of shockwaves used and auxiliary procedures. To analyze the data, statistical package for a social science (SPSS) 23 was used; Chi-squared, Mann Whitney U test, and cross-tabulations tests were performed to identify the significance of data.
This study includes 194 patients with stone disease; the demographic data of enrolled patients were represented as gender distribution and mean age. Male participants of the study were 136(70.1%) and 58(29.9%) were females with mean age and standard deviation (SD) of 42.7±14.2 years (Table 1).
Table 1: Demographic data for extra corporeal shockwave lithotripsy (ESWL) particulars.
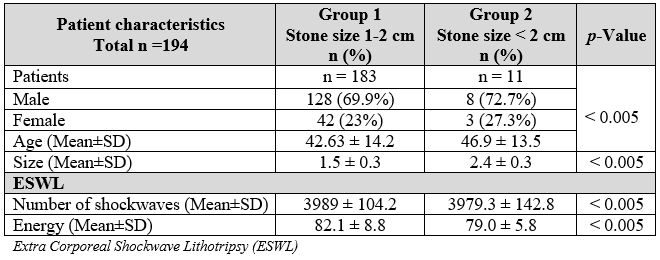
Subdivision of groups according to the stone size and DJ stenting along with SFR (stone-free rates) were analyzed and slight differences were recorded between stone-free rates of patients with DJ stenting n=83 (42.7%) and patients without DJ stents n=87(44.8%) respectively. The stones n=14 (7.2%) were recorded as partially cleared in patients with DJ stents while n=10(5.1%) showed partial clearance without DJ stents (Table 1). Although the auxiliary procedures documented were higher in stented group with 09 out of 97 patients were recorded. Patients needed ureteroscopy for urolithiasis (URS) with extracorporeal shock wave lithotripsy, while 1 patient needed percutaneous lithotripsy for complete stone clearance, the patient underwent PCNL recorded multiple renal stones, 04 patients needed DJ stent insertion after Extracorporeal shock wave lithotripsy (Table 2), the requirement of sessions for complete stone clearance highly depends upon the stone size. The bigger the stone the more session are required to break it. Large stones are reportedly more prone to complications such as hematuria and loin pain (Table 2).
Table 2: Extracorporeal shock wave lithotripsy (ESWL) and its related parameters.
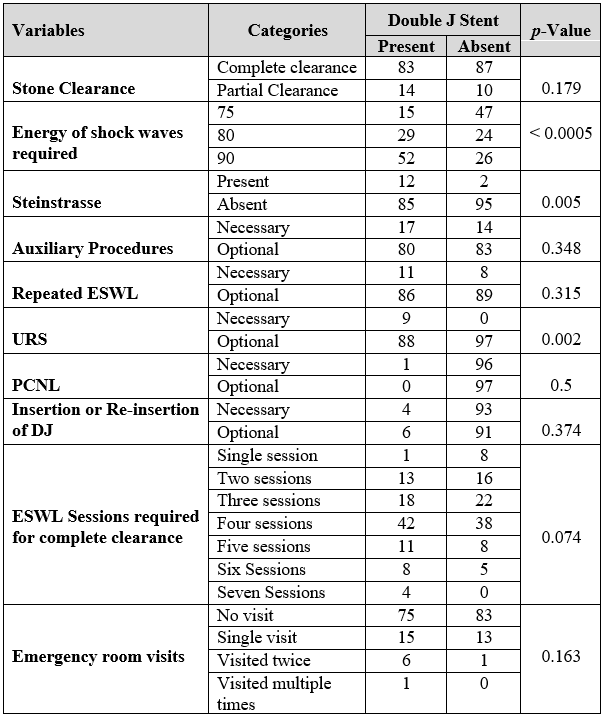
Extra Corporeal Shockwave Lithotripsy (ESWL); Micro Percutaneous Lithotripsy (PCNL), Ureteroscopy (URS)
Our study showed an immense difference between post-operative complications of stented and non-stented groups, the reported complications and emergency ward visits were enhanced after double J stent placement, the most common complaint was mild to moderate Hematuria and Pain. The significance of DJ stent after extra corporeal shockwave lithotripsy (ESWL) for renal stones is doubtful; our investigations reported no help in renal stone passage after placing DJ stent post ESWL. In this study, Group II reportedly showed better results in order of stone passage and fewer complications. Ureteral stents are helpful after ureteroscopic stone removal for smooth stone passage; the rationales instigate by hypothesis rather than evidence-based studies.
Although the DJ stent use after many urologists previously adopted ESWL, its routine use is presently unsettled due to excessive stent-related symptoms. The placement of a Ureteral stent / DJ stent has an association of patient’s significant morbidity, enhances financial burden to the patient of stent removal unless pull string stent is used15. Avoiding the stent can decrease procedure costing and operating room space, improve pain management and avoiding unnecessary emergency room visits are also important factors to reduce the financial burden. Some of the trails shared similar complications post operatively, therefore, numerous similarities with our study including uncomplicated procedure, Urethral dilation absence etc. However, in the literature, there are no differences found in hospitalized and recovered patients after the stenting procedure16,17. Ureteral stents are associated with major symptoms including pain, LUTs, and reduced working capacity, which results in reduced quality of daily life, whereas ureteral stents, may cause pain and LUTs specifically dysuria, urgency and mild to moderate hematuria18-22.
Another study of 20 patients with DJ stent and the reported complications stated 90% positive results with one or more than one reported stent related Lower urinary tract symptoms23. A study reported pain after SWL stent placement in 44% of patients along with dysuria, urgency and increased use of analgesia, which was subsided after stent removal24. A DJ stent, which was forgotten for four years in 40 years old female showed sepsis in ER, the severely encrusted DJ stent was then removed, and patient get symptom free25. Forgotten stent are responsible to cause severe morbidity in pediatric population along with UTI, hematuria and encrustation of stent resulting in obstruction26. Stents strongly affect mental and physical health and cause pessimistic force on functional capability and work performed during the first post-operative weeks, patients with stent placement showed more consumption of pain relief medications orally than non-stented patients27.
Another potentially serious complication of SWL is steinstrasse; the incident of the steinstrasse has been reportedly increased after DJ insertion prior to SWL by 4.6% 28. Similar findings have been revealed in various other studies. Irritation and discomfort can be associated with stent length and placement of distal loop. Ureteral stent with elongated distal end may results in bladder symptoms, such as frequency and urgency29. Routine placement of indwelling results showed clear insignificance of stone-free rates between DJ stented group and non-stented group. The use of double J stent for Ureteral stone removal or decreasing hydronephrosis is really popular from decades, improved design and maintaining its side effects make DJ stent an ideal friendly procedure although it has quite unfriendly consequences after a certain time period if not removed. Forgotten DJ stent is a very common and serious condition in countries like Pakistan, encrusted DJ, enlarged stone burden are common side effects30. The ureteral stent should be removed before incrustation; removing a highly incrusted DJ stent can cause urothelium, injuries, consecutive strictures, bleeding, impossible stent removal or ureter avulsion.
Unplanned ER visits were significantly higher in the stented group as compared to non-stented due to acute flank pain and moderate hematuria after ESWL. Many urologists avoid the use of Stent with a stone size of < 2.0 cm while a large number of urologists still use DJs after SWL20. In other studies, it is defined that use of a stent is not beneficial with stones even larger than 1.0 cm. Moreover, our study confirmed these reports and concluded that stents do not interfere with stone-free rates after ESWL but enhance the stent-related complications such as steinstrasse and discomfort18-23. We recommend that routine usage of DJ stent after every ESWL should be minimized and only selected patients get DJ stenting after ESWL.
The stone-free rates were found higher in the group without DJ stent. DJ stent used to enhance stone-free rates was not beneficial and stone-free rates were not affected by the presence of stent. This might raise the chances of developing complications such as stent related side effects, LUTs, dysuria and loin pain.
The authors would like to acknowledge the staff of Liaquat University of Medical and Health Sciences, Jamshoro for their support in data collection.
The authors declare no conflict of interest.
The study was approved from Institutional Research Committee of the Kidney Center, Karachi Pakistan. Reference number of TKC-ERC was 32(A)-URO-072015.
Informed consents were taken from every patient.
WM was the primary author with the idea and objective for the study. SK and IS assisted in generating questionnaire. SS helped in maintaining the data confidentiality, analysis while AH, AU assisted in data entry, and ST assisted in research write up and analysis.
- Bangash K, Shigri F, Jamal A, Anwar K. Spectrum of renal stones composition; chemical analysis of renal stones. Int J Pathol. 2011;9(2):63-66.
- Polat H, Yücel MÖ, Utangaç MM, Benlioğlu C, Gök A, Çift A, et al. Management of forgotten ureteral stents: relationship between indwelling time and required treatment approaches. Balkan Med J. 2017;34(4): 301-307.
- Türk C, Petřík A, Sarica K, Seitz C, Skolarikos A, Straub M, et al. EAU guidelines on interventional treatment for urolithiasis. Eur Urol. 2016;69(3):475-482
- Chew BH, Seitz C. Impact of ureteral stenting in ureteroscopy. Current opinion in urology. 2016 Jan 1;26(1):76-80.
- Sharma A, Andankar M, Pathak H. Two cases of retained ureteral stents presenting with breakage and encrustations. Int J Med Res Health Sci. 2018;5(10):208-212.
- Badawy AA, Saleem MD, Abolyosr A, Aldahshoury M, Elbadry MS, Abdalla MA, et al. Extracorporeal shock wave lithotripsy as first line treatment for urinary tract stones in children: outcome of 500 cases. Int Urol Nephrol. 2012;44(3):661-666.
- Finney RP. Experience with new double J ureteral catheter stent. J Urol. 1978;120(6):678-681.
- Sharma R, Choudhary A, Das RK, Basu S, Dey RK, Gupta R, et al. Can a brief period of double J stenting improve the outcome of extracorporeal shock wave lithotripsy for renal calculi sized 1 to 2 cm? Investig Clin Urol. 2017;58(2):103-108.
- Libby JM, Meacham RB, Griffith DP. The role of silicone ureteral stents in extracorporeal shock wave lithotripsy of large renal calculi. Journal Urol. 1988;139(1):15-17.
- Lang EK. Diagnosis and management of ureteral fistulas by percutaneous nephrostomy and antegrade stent catheter. Radiol. 1981;138(2):311-317.
- Bierkens AF, Hendrikx AJ, Lemmens WA, Debruyne FM. Extracorporeal shock wave lithotripsy for large renal calculi: the role of ureteral stents. A randomized trial. J Urol. 1991;145(4):699-702.
- Payne SR, Ramsay JW. The effects of double J stents on renal pelvic dynamics in the pig. J Urol. 1988 Sep;140(3):637-641.
- Jones BJ, Ryan PC, Lyons O, Grainger R, McDermott TE, Butler MR. Use of the double pigtail stent in stone retrieval following unsuccessful ureteroscopy. Br J Urol. 1990;66(3):254-256.
- Musa AA. Use of double-J stents prior to extracorporeal shock wave lithotripsy is not beneficial: results of a prospective randomized study. Int Urol Nephrol. 2008;40(1):19-22.
- Ozkan B, Dogan C, Can GE, Tansu N, Erozencı A, Onal B. Does ureteral stenting matter for stone size? A retrospective analyses of 1361 extracorporeal shock wave lithotripsy patients. Cent European J Urol. 2015;68(3): 358-364.
- Joshi HB, Okeke A, Newns N, KeeleyJr FX, Timoney AG. Characterization of urinary symptoms in patients with ureteral stents. Urol. 2002;59(4):511-516.
- Obaid AT, Hussen RF. Role of double J stent in patients with renal stones undergo extracorporeal shock wave lithotripsy. Med J Babylon. 2012;9(3):629-642
- Chaussy CG, Tiselius HG. How can and should we optimize extracorporeal shockwave lithotripsy? Urolithiasis. 2018;46(1):3-17.
- Prstojevic JK, Junuzovic D, Hasanbegovic M, Lepara Z, Selimovic M. Characteristics of calculi in the urinary tract. Mater Sociomed. 2014;26(5): 297-302.
- Kwon JK, Cho KS, Oh CK, Kang DH, Lee H, Ham WS, et al. The beneficial effect of alpha-blockers for ureteral stent-related discomfort: systematic review and network meta-analysis for alfuzosin versus tamsulosin versus placebo. BMC Urol. 2015;15(1):1-10.
- Dauw CA, Simeon L, Alruwaily AF, Sanguedolce F, Hollingsworth JM, Roberts WW, et al. Contemporary practice patterns of flexible ureteroscopy for treating renal stones: results of a worldwide survey. J Endourol. 2015;29(11):1221-1230.
- Chauhan VS, Bansal R, Ahuja M. Comparison of efficacy and tolerance of short-duration open-ended ureteral catheter drainage and tamsulosin administration to indwelling double J stents following ureteroscopic removal of stones. Hong Kong Med J. 2015;21(2):124-130.
- Pollard SG, Macfarlane R. Symptoms arising from Double-J ureteral stents. J Urol. 1988;139(1):37-38.
- Reddy S, Kulshreshtha M, Singh P. A prospective study comparing stenting versus non-stenting after uncomplicated ureteroscopy for ureteric stones. J Evol Med Dent Sci. 2016;5(61):4291-4295.
- Prihadi JC, Kusumajaya C. Double-J stents forgotten for four years: a case report. Med J Indones. 2019;28(3):280-283.
- Nerli RB, Magdum PV, Sharma V, Guntaka AK, Hiremath MB, Ghagane S. Forgotten/retained double J ureteric stents: A source of severe morbidity in children. African Afr J Paediatr Surg. 2016;13(1): 32-35.
- Joshi HB, Stainthorpe A, MacDonagh RP, Keeley FX, Timoney AG. Indwelling ureteral stents: evaluation of symptoms, quality of life and utility. J Urol. 2003;169(3):1065-1069.
- Sulaiman MN, Buchholz NP, Clark PB. The role of ureteral stent placement in the prevention of Steinstrasse. J Endourol. 1999;13(3):151-155.
- Musa AA. Use of double-J stents prior to extracorporeal shock wave lithotripsy is not beneficial: results of a prospective randomized study. Int Urol Nephrol. 2008;40(1):19-22.
- Kandemir A, Sönmez MG. Treatment of fragmented and severely encrusted ureteral double-J stent forgotten for 11 years through multimodal endourological methods. Urol Ann. 2019;11(3): 310-313.
This is an open-access article distributed under the terms of the CreativeCommons Attribution License (CC BY) 4.0 https://creativecommons.org/licenses/by/4.0/