By Naseer Ahmed1, Abhishek Lal2, Maha Shakeel2, Danish Cyrus2, Fatima Tuz Zehra2, Ahsan Ayub2
AFFLIATIONS:
- Department of Community Dentistry, Altamash Institute of Dental Medicine, Karachi, Pakistan.
- Student, Altamash Institute of Dental Medicine, Karachi, Pakistan.
ABSTRACT
Background: Exodontia is one of the most frequently carried out procedures by a dental surgeon, mostly on an outpatient department basis. The reasons for performing exodontia include non-restorable teeth, periodontal disease, dental trauma, impacted tooth, orthodontic treatment and toothache. Complications in dental extraction are a commonly encountered problem in dental clinics. This knowledge can help dental surgeons make extractions less invasive, traumatic and complicated, enabling quicker recovery of the socket. The aim of this study was to recognize types, frequency and risk factors for complications after exodontia.
Methods: This cross-sectional study enrolled patients who had exodontia done from July- September 2019, visiting OPD of the Oral surgery department of Altamash Institute of Dental Medicine, Karachi. Risk factors included demographic data, general health, past medical and dental history. Spearman’s correlation test was used to establish any relationship of variables with complications.
Results: The study patients (126) included 72 females (mean age 39.1±13.39) and 54 males (mean age 41.1±14.93). The overall complications rate was found to be 7.1%, mainly arising from maxillary and mandibular third molars. The most common complications encountered were Hemorrhage, Pain, and Trismus. Increasing age and specific teeth extracted were associated with an increased risk for complications. However, post-operative complications which were encountered most of them were minor and handled on an outpatient department basis.
Conclusion: Frequency and risk factors for complications after exodontia were found low3 (37.5%). While age and teeth extracted cannot be directly altered, these factors maybe indirectly modified, resulting in a potential decrease of postoperative complications.
Keywords: Oral Surgery, Exodontia, Complications.
Exodontia, also known as dental extraction is a procedure whereby one or more than one tooth is extracted out of their sockets. There are many reasons for the dental surgeon to perform exodontia which includes severe dental pain, non-restorable tooth, periodontal disease, carious teeth, dental trauma, retained deciduous teeth, increase mobility, a patient requiring dentures, dental abscess, orthodontic treatment, impacted tooth and sometimes teeth associated with tumors1,2.
Dental extraction can be performed using two different approaches. First is called closed extraction, where only dental forceps and elevators are used to extract the teeth out of their sockets with no elevation of the flap3. The second approach is called open extraction or surgical extraction where the flap is raised surgically using a scalpel and adjunctly bone is drilled using a hand piece with forceps and elevators also being used4. Indications for both closed and open extractions are different from the initial approach usually being closed. Certain indications make open extractions the first choice, which includes impacted teeth, unusual root morphology, and dilacerations of root tips along with ankylosed tooth, hypercementosis, and teeth lying close to vital structures4.
Exodontia, one of the commonest procedures performed in dental practice, can be associated with postoperative complications with significant biological and social impact. Complications are unfortunate events that tend to increase morbidity, more than what would be expected from a specific operative procedure in normal circumstances2. Although they are uncommon, their happening leads to a prolonged period of treatment, which is uncomfortable for the patient as well as the dental surgeon. Thus, careful attention to detail is required which includes a detailed case history, routine investigations; for example, radiographs and blood tests are a core part of exodontia5.
Complications are part of almost every procedure that a dental surgeon can perform but some procedures are more prone to complications than others are, exodontia is one of them. Experienced dental surgeons do anticipate and many times are prepared for such circumstances which if taken care of before the procedure usually leads to an uneventful procedure, no complications postoperatively, and no additional follow-ups for the patients4.
So, preoperative assessment of unchangeable risk factors includes age5,6, gender, medical history of patients such as conditions associated with wound healing problems (that is chronic hepatitis), diabetes, hypertension, blood dyscrasia (hemophilia, thalassemia) or drug-induced reactions were also considered risk factors leading to complications after exodontia7,8. Moreover, factors considered modifiable are the use of tobacco, oral hygiene, and oral contraceptives.
Anticipated (clinically and radiologically) potentials intra-operative risk factors of exodontia are, dental surgeon’s experience, the time duration of surgery, the technique of anesthesia administration, intrasocket medications, and topical anesthesia9,10. Finally, post-operative, early and late, complications commonly encountered include pain, swelling, trismus, hemorrhage, dysesthesia, severe infection, fracture, dry socket, damage to adjacent teeth, and displaced teeth. Most of these complications are temporary but some are permanent which may lead to a functional deficit. The main objectives of this investigation were to identify risk factors associated with post-operative complications as well as the types and frequency of complications after extractions.
The study design was cross-sectional using random sampling to collect data. The study subjects were recruited from patients at Altamash Institute of Dental Medicine, Karachi, Pakistan OPD between July 2019 to September 2019. The patients who had one or more dental extractions with evidence of post-operative follow up were included to access outcomes. Patients presenting to the OPD with co-morbidities such as hypertension, diabetes, hepatitis, blood dyscrasias were also included. Patients without evidence of post-operative follow-up were excluded from the sample. The Ethics Review Committee of Altamash Institute of Dental Medicine approved this study (AIDM/EC/06/2019/10).
The predictor variables, that is, risk factors or exposure were grouped into the following settings of variables: demographic, medical and dental history, anatomic, and operative. Before performing surgery, the evaluation included a medical and dental history of the patients, personal information including name, gender, age, education, occupation, residence, and marital status.
Patients with a positive medical history that might affect immunity or contraindicate surgery e.g., cardiovascular diseases, diabetes mellitus, bleeding disorders, liver or kidney dysfunction, respiratory ailment, hepatitis B or C were part of this study. A positive dental history was recorded in the following circumstances: teeth sensitivity, bleeding gums, orthodontic treatment, and difficulty in moving jaws, mobile teeth, and bruxism. The consumption of tobacco, betel nut, and naswar (powdered tobacco) was also taken into account. The presence or absence of postoperative complications after performing exodontia was the primary outcome variable with risk factors associated with postoperative complications and their frequencies being the secondary outcomes of the study.
After extractions were carried out occurrence of the following complications were observed: pain, swelling, trismus, hemorrhage, damage to adjacent teeth, displaced teeth, infection, ulceration, dry socket, and fracture. For statistical analysis, SPSS was used. For correlation between variables, Bivariate analysis was used to compare variables which include age, gender, medical history, dental history, habits, location of extraction and teeth extracted were compared with the occurrence of complications after exodontia was performed. Spearman’s statistical test was used to perform this analysis and a p-value of ≤0.05 was considered statistically significant.
The results indicated that between the months from July to September 2019, a total of 126 patients, consisting of 72 (57.1%) females and 54 (42.9%) males who visited the Oral Surgery Department, who had one or more teeth extracted by a Dental Surgeon were finalized. The sample’s mean average age was 39.1±13.39for females and 41.1±14.93for males. Descriptive Statistics are shown in Table 1.
Table 1: Frequency of different teeth extracted in maxilla and mandible.
| Kinds of Teeth | Teeth in Females
n (%) |
Teeth in Males
n (%) |
| Maxillary Anteriors | 5(5.1) | 7(9) |
| Maxillary Posteriors | 45(46) | 24(30.7) |
| Mandibular Anteriors | 5(5.1) | 8(10.3) |
| Mandibular Posteriors | 43(43.8) | 39(50) |
Anteriors: Central incisor to canine, Posteriors: First premolar to third molar.
Among 126 patients, a total of 176 teeth were extracted. Of these 176 extracted teeth, 172(97.8%) closed or non-surgical approach was used to extract the teeth and only 4 (2.2%) teeth required surgical or open extraction approach. 46 (26.1%) extractions were third molars. Patients belonging to the age group of adults and the elderly mainly had their teeth extracted with a smaller number of adolescent and children patients. Patients with a positive medical history were 45 (35.7%). Hypertension and Diabetes were the most common positive factors among recruited patients’ medical history. A small number of patients reported having a positive medical history of arthritis, asthma, tuberculosis, and thyroid problems (Table 2).
When these variables of age, gender, medical history, dental history, habits, location of extraction, and teeth extracted were entered in bivariate Spearman’s test analysis for correlations, they had an association with the occurrence of complications (Table 2). As the age of the patient increases, the occurrence of complications increases (p-value=0.02). A similar relationship was also seen with teeth extracted (p-value=0.04). Variables, which had no effect on occurrence of complications, include gender (p-value=0.25), medical history (p-value=0.16), dental history (p-value=0.51), habits (p-value=0.92) and location of extraction (p-value=0.41) as shown in table 2.
Table 2: Significance of variables in relation to complications.
| Parameters | Correlations with Exodontia | p-Value |
| Age | -0.40** | 0.00 |
| Gender | 0.08 | 0.37 |
| Medical History | 0.18* | 0.04 |
| Dental History | -0.09 | 0.33 |
| Habits | -0.23** | 0.01 |
| Location of teeth | -0.09 | 0.30 |
| Complications | -0.18* | 0.04 |
Considering the habits of the patients, smoking, paan/gutka, and betel nuts consumption was frequently encountered with a small number of naswarusages. In our study, the major cause of performing dental extractions was pain. A small number of patients with caries, mobility swelling gums, missing tooth, sensitivity, trauma, retained deciduous teeth, patient wish, loose denture, extraction needed, and prostheses needed also required dental extraction to be performed (Figure 1).
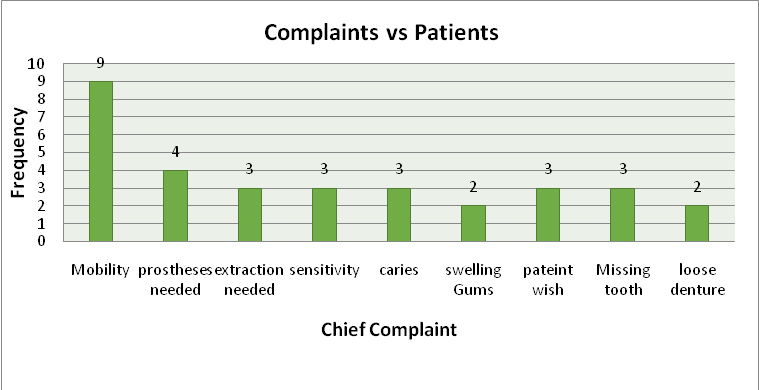
Figure 1: Assessment of chief complaints of the patients.
Teeth most frequently extracted were in the posterior segments of both maxilla and mandible i.e., the molars and they were generally extracted under local anesthesia. In two exceptional cases, general anesthesia was required, although no complications were reported among them. The number of teeth extracted in the anterior segment of both maxilla and mandible was less. There was no use of preoperative antibiotics. In our study, no complication of adjacent tooth damage, ulceration, a displaced tooth, infection, dry socket, and fracture was reported. All of the reported complications were found in teeth undergoing closed extraction, with no complications arising from open extractions. In types and frequencies of postoperative complications after exodontia, most frequently encountered complications after extractions were pain, trismus, and hemorrhage. There was no case of damage to neither lingual nerve nor the inferior alveolar nerve. Post-operative complications that were encountered most of them were minor and handled on an outpatient department basis.
Of the 8 patients in whom complications postoperatively were found, 3 (37.5%) of them had a positive medical history of diabetes, asthma, thyroid problems, and hypertension. The majority of these patients were females belonging to the age group of adults. None of these patients consumed tobacco, alcohol, betel nut, or naswar. Considering gender, complications mainly arose in females. Of a total of 98 teeth extracted in females, complications were found in the extraction of 12 (12.2%) teeth mainly molars. On the other hand, in males of the total of 78 teeth extracted, the complication was found in 1 (1.3%) tooth which was a maxillary third molar. Except for two cases, all of the above-mentioned dental extractions were performed under local anesthesia. No case was reported of using preoperative antibiotics. Patients who did not come for follow-up were excluded from this study.
The overall complication rate in the study was 7.1%. Besides, the majority of the complications were related to molars, particularly third molars11,12. The investigation outcomes concluded trismus and pain as the most frequently encountered complications. Teeth that are most commonly extracted includes mainly third molars, with anterior dentition both in maxilla and mandible being less frequently extracted13,14.
Extractions were performed on the patients mainly because the tooth had an unfavorable prognosis for restorative treatment with extraction then being the most likely outcome. Patients present to the dental surgeon quite late when saving the tooth becomes less likely as compared to patients frequently visiting the doctor at least once or twice a year normally. The complication rate in the study is within the range reported in the referenced literature. Studies similarly concluded results corresponding to this study, although there was no presentation of dry socket (Alveolar Osteitis) during the determined duration of this study in literature, the dry socket has been documented15,16.
Almost all of the post-op extraction complications were present in females with the adult age group17. Males had significantly a smaller number of complications18. Consistent with the previous studies, the most common complications after exodontia was associated with third molars19,20. Post-operative extraction complications these days tend to be less frequently encountered in OPD mainly because of better techniques used for extractions, the doctor’s understanding of the complications, how they can be avoided, better treatment of the complications if encountered, and how to prevent them. In our study, we encountered pain, trismus, and hemorrhage as the most frequently occurring complications19,21. whereas, in the literature, the most frequently occurring complications include post-operative pain, hemorrhage, dry socket and infection7,22.
The second objective of our study was to identify any risk factors associated with post-operative extraction complications. We concluded from our data, age and teeth extracted were contributing factors that might lead to complications. Although at times, there is insufficient data to make a judgment regarding these mentioned risk factors23.
Hypertension and Diabetes were found to be the most frequently encountered medical condition of patients visiting the OPD and the complications were also found in these patients after exodontia making both of these conditions potential risk factors for complication post extractions24. Although no significant relationship can be concluded from our data as complications of trismus and pain were found in one patient who was diabetic. Patients frequently have been positive for dental history mainly gingivitis and periodontitis, but its presence does not predispose patients to postoperative complications as we found in this study.
In the current study, age correlates and acts as a risk factor for post-operative extraction complications25. Although different results regarding age is mentioned in the literature16. This positive correlation could be due to an increase in bone density as a person ages and this leads to difficulty in extraction, which in turn increases the chances of complications particularly in third molars. A medical history may also be a contributing factor in complications mainly because of patients not keeping in check their health like maintaining blood pressure and blood sugar levels. This study did not find any positive correlation of patients with a positive social history of e.g. smoking, pan, betel nut and naswar with post-op complications, although tobacco is often a very well documented factor in literature23,25. Gender and age are often considered as positive factors for complications.
Pain and stress are documented to positive risk factors associated with post-operative exodontia complications23. Therefore, varying from patient to patient; anxiety should be taken care of as this will decrease procedure duration, extraction will be less traumatic, and exceeding cartridges of local anesthesia will not be required. All these factors are known to be of hindrance during the procedures. Several methods are able including intravenous sedation and administration of various drugs available usually a few hours before the procedure or the night before25. In this study, complications that occur after exodontia have been reported. One of the limitations is that the study included a smaller sample size. Another is that it would have been better if other relatable risk factors regarding complications after exodontia were also included in this study.
The frequency and risk factors for complications after exodontia were found low. While age and teeth extracted cannot be directly altered, these factors maybe indirectly modified. It is of vital importance that a dental surgeon recognizes the complications that occur or might occur so that it can be handled accordingly. Dental surgeons must recognize the impending complications and manage them accordingly
The authors would like to acknowledge all the participants that were part of this study.
The authors declare no conflict of interest.
The Ethics Review Committee of Altamash Institute of Dental Medicine approved this study (AIDM/EC/06/2019/10).
Verbal and written consent were taken from the participants.
NA provided his valuable guidance and interpreted the patient’s data. AL collected data, literature review, made figures and was a major contributor in writing the manuscript. AA collected data and provided his knowledge in writing the manuscript. DC collected data and formed tables. FTZ collected data and conducted a final revision of the article. MS also collected data and responsible for data management.
- Taiwo AO, Ibikunle AA, Braimah RO, Sulaiman OA, Gbotolorun OM. Tooth extraction: Pattern and etiology from extreme Northwestern Nigeria. Eur J Dent. 2017;11(03):335-339.
- Mamoun J. Use of elevator instruments when luxating and extracting teeth in dentistry: clinical techniques. J Korean Assoc Oral Maxillofac Surg. 2017;43(3):204-211.
- Jennifer Archibald D. What to know about tooth extraction [Internet]. [cited 2020 Aug 11]. Available from: https://www.medicalnewstoday.com/articles/327170
- Deliverska EG, Petkova M. Complications after extraction of impacted third molars-literature review. Annu Proc Sci Papers. 2016;22(3):1202-1211.
- Osunde OD, Saheeb BD. Effect of age, sex and level of surgical difficulty on inflammatory complications after third molar surgery. J Maxillofac Oral Surg. 2015;14(1):7-12.
- Khosla A, Venkateshwar G, Padhye M, Kakkar S. Complications of exodontia: A retrospective study. Indian J Dent Res. 2011;22(5):633-638.
- AlHindi M. Dry socket following teeth extraction: effect of excessive socket saline irrigation. J Oral Heal Dent Sci. 2017;1(1):1-5.
- Azam K, Hussain A, Maqsood A, Farooqui WA. Effects of surgery duration on post-extraction sequelae following impacted third molar surgery by using two different bone cutting methods; a double blind randomized trial. Pak Oral Den J. 2016;36(1):1-1.
- Azam AN, Ezoddini F, Khalesi M, Gholami L, Momtaz A. Evaluation of the complications after mandibular third molar surgical extraction. Avicenna J Dent Res. 2018;2(1):23-28.
- Sayed N, Bakathir A, Pasha M, Al-Sudairy S. Complications of Third molar extraction: A retrospective study from a tertiary healthcare centre in Oman. Sultan Qaboos Univ Med J. 2019;19(3):e230-e235.
- Normando D. Third molars: To extract or not to extract? Dental Press J Orthod. 2015;20(4):17-18.
- Rakhshan V. Common risk factors of dry socket (alveolitis osteitis) following dental extraction: A brief narrative review. J Stomatol Oral Maxillofac Surg. 2018;119(5):407-411.
- Mahomed VM and O. Incidence and predisposing factors for dry socket following extraction of permanent teeth at a regional hospital in Kwa-Zulu Natal : Research. South African Dent J. 2016;71(4):166-169.
- Ahmed A, Mohamed F, Hattab K. Surgical extraction of impacted mandibular third molars: postoperative complications and their risk factors. Jamahiriya Med J. 2009;9(4):272-275.
- Farshid A, Mohiti A, Ghasemzadeh O. Prevalence and risk factors for complications of mandibular third molar surgery. Am J Oral Maxillofac Surg. 2015;2(1):43-52.
- Malkawi Z, Al-Omiri MK, Khraisat A. Risk indicators of postoperative complications following surgical extraction of lower third molars. Med Princ Pract. 2011;20(4):321-325.
- Sigron GR, Pourmand PP, Mache B, Stadlinger B, Locher MC. The most common complications after wisdom-tooth removal: part 1: a retrospective study of 1,199 cases in the mandible. Swiss Dent J. 2014;124(10):1042-1056.
- Miclotte I, Agbaje JO, Spaey Y, Legrand P, Politis C. Incidence and treatment of complications in patients who had third molars or other teeth extracted. Br J Oral Maxillofac Surg. 2018;56(5):388-393.
- Kumar MA, Gheena S. Incidence of dry socket after third molar extraction. J Pharm Sci Res. 2015;7(7):451-452.
- Huang S, Dang H, Huynh W, Sambrook P, Goss A. The healing of dental extraction sockets in patients with Type 2 diabetes on oral hypoglycaemics: a prospective cohort. Aust Dent J. 2013;58(1):89-93.
- Trybek G, Chruściel-Nogalska M, Machnio M, Smektała T, Malinowski J, Tutak M, et al. Surgical extraction of impacted teeth in elderly patients. A retrospective analysis of perioperative complications – the experience of a single institution. Gerodontol. 2016;33(3):410-415.
- Kapil A, Rohit P, Neha P, Neetu A, VikasB. Complications and risk factor associated with extraction of impacted third molars: A prospective study. Int J Contemp Med Surg Radiol. 2017;2(4):153-155.
- Bortoluzzi MC, Capella DL, Barbieri T, Marchetti S, Dresch CP, Tirello C. Does smoking increase the incidence of postoperative complications in simple exodontia? Int Dent J. 2012;62(2):106-108.
- Schwartz-Arad D, Lipovsky A, Pardo M, Adut O, Dolev E. Interpretations of complications following third molar extraction. Quintessence Int. 2018;49(1):33-39.
- McDowall C, Lydall ES, Moore SC. The potential role of patient stress in rates of dental post-extraction complication. Oral Surg. 2014;7(3):162-167.
This is an open-access article distributed under the terms of the CreativeCommons Attribution License (CC BY) 4.0 https://creativecommons.org/licenses/by/4.0/