By Munazza Suharwardy Obaid1, Saeed Minhas2, Fouzia Naeem Effendi3, Shiraz Shaikh4, Farah Fatima Abbas5, Ferrukh Zehravi6, Malik Tajuddin1, M Bastle Ullah Ansari7
AFFLIATIONS:
- Department of Community Medicine, Dow University of Health Sciences, Pakistan and Visiting Academic in Manchester University.
- Department of Surgery, Jinnah Post Graduate Medical Center, Karachi, Pakistan.
- Department of Community Health Sciences, Bahria University Medical and Dental College, Karachi, Pakistan.
- Department of Public Health, Jinnah Sindh Medical University, Karachi, Pakistan.
- Department of Pathology, Dow University of Health Sciences, Karachi, Pakistan.
- Department of Community Medicine, Liaquat National Medical College, Karachi, Pakistan.
- Student, Karachi, Pakistan.
ABSTRACT
Background: Injury is a significant issue of public health, a major global burden and first aid training programs incorporated as part of school curriculum will have a considerable impact on public health, and this will in turn reduce out of hospital cardiac arrests. The study aimed to determine the immediate First aid knowledge and long term retention of its knowledge (after three months) of the students (13-18 years), participating in a volunteer program in Karachi.
Methods: This study was conducted in a tertiary care hospital, delivering First aid training to 143 participants by Basic life support (BLS) trained staff in a tertiary care hospital. The design consisted of a pre-test, post-test and follows up assessments, carried out via questionnaire and hands-on assessment. SPSS was used for statistical analysis. ANOVA and Friedman test was applied to evaluate the dependent variable’s improvement in knowledge between pre, post and follow up tests.
Results: From 143 participants, 41.5 %, 63.8 % and 61 % satisfactory results were seen in the pre-test, post-test and follow up assessments, respectively. In Pre-test, males scored 18.75 % and the females scored 8.42%, whereas, in the post-test, the scores were 75.7% and 64.58% respectively. Similarly, in follow up evaluations results obtained were 62.1% and 45.8% respectively. Hands-on scores were 88.4% in males and 95.8 % in females.
Conclusion: The level of first aid knowledge was unquestionably less satisfactory in the pre-test evaluations compared to post-test and follows up assessments. Due to its effectiveness, it should be incorporated as part of the school curriculum.
Keywords: Adolescents; Knowledge; Cardiopulmonary Resuscitation.
When an injury or an illness occurs to a victim, the help and assistance provided by a layperson or trained one, until a definitive medical treatment arrives, is called first aid (FA) 1. FA includes Basic life support (BLS) which comprises of initial assessment, airway maintenance, and expired air ventilation and chest compressions and is known as cardiopulmonary resuscitation (CPR) 2.
First aid is a huge terminology but some components of first aid skills would include CPR and immediate care of fractures, poisoning, burns of all degrees etc 3. The eventual goal of first aid is to stop or abolish the possible damage at a given time before reaching a suitable health care centre; consequently, it is important to give fundamental knowledge of first aid to all4.
Throughout the world, injury is the major killer of children as well as adolescents and accounts for approximately 133,117 deaths in Electronic medical records (EMR) compared to 707,755 globally5. First aid provided by the local people can reduce the death toll significantly6. FA can be taught from a very young age to school going children7. In developed countries, FA is part of the curriculum as students are a good source of transforming information to the community. It has been noticed that high school children are more prone to injuries and have an affinity to be involved in riskier attitudes towards life 2,8. Prompt response at the right time can save a lot of lives and affect future health and quality of life as well 9.
It has been suggested, training for bystanders has been a means of bridging the gap in localities with inadequate Emergency medical services10. General public education campaigns should be encouraged in this field11. Research in Pakistan suggested the adolescent age group can be of great help for the family members and can call for help in case of emergency to reduce casualties12. Another study from Pakistan quoted that 17.5 % of students have had formal first aid training showing (p-value <0.001) when the comparison was made between trained and non-trained students in answering correctly13.
In all public settings, first aid measures are an important service that should be provided. In educational services, it is imperative to be able to provide prompt basic first aid14. The health problem of a society can be addressed if the students can be appropriately prepared and cultured for healthful living as they have great potential15. Hence, this study explored the level of knowledge of the above-mentioned age group along with this it would provide a baseline survey as well as give an update about the improvement brought in because of the intervention. This study would help us evaluate their knowledge about how to resuscitate airway and breathing passage to reduce the morbidity, mortality, and disability due to unintentional injuries. This would also sensitize them with the basic skills and give the confidence to respond in an emergency. This study will develop an evidence-based educational pathway to enable the integration of first aid into the school curriculum by defining the goals to train different age groups. The study aimed to determine the immediate first aid knowledge and long term retention of its knowledge (after three months) of the students 13-18 years old participating in a volunteer program in Karachi.
This quasi-experimental study with the intervention of a first aid /Basic Life Support training program was conducted in a tertiary care hospital. The 13-18 years old students were included in the study. Two groups of 25 students were randomly selected from three batches and were trained by the hospital’s specially trained Basic life support (BLS) staff. The sample size of 137 was calculated using the software to cater for non-response, incomplete questionnaires, or drop out from the study 10% was added and the final sample size was 150.
The volunteer program took 6 days; the intervention was given in the first two days from 9.30am to 12pm. A pre-test was done on the first day of the training and post-test was conducted at the end of the second day after the intervention was completed. Data collection was done with the help of the hospital team as well as the principal investigator. Participants’ informed consent was taken from the student’s parents. Ethical approval was obtained from the hospital administration to conduct the research and intervention and the IRB reference number was JSMU/IRB/2017/-89.
A questionnaire was used for Assessment of the Victim (6), CPR (11), Breathing (6) and information regarding the infant’s assessment (3). Experts and Cronbach’s Alpha calculation (0.762) validated the questionnaire. Based on the panel of experts the participant’s knowledge was considered satisfactory when the total score was 60% or more and unsatisfactory when it was less than 60 % 16. SPSS was used for data entry and statistical analysis. In order to compare the three groups repeated ANOVA was used. Friedman test was applied as data were not normally distributed, to evaluate the dependent variable’s improvement in knowledge between pre, post and follow up tests and p < 0.05 was considered statistically significant.
A total of 150 students were given a questionnaire at three different stages pre-test (before the intervention), post-test 1 (after the intervention), follow up and assessment (after three months). Valid responses collected at the end were 143 making a response rate of 95.3 %. The average age (Table 1) of the participants was (mean±SD) 15.92±1.24 of which 95.9% of the students belonged to matric/O’levels, 35.3% belonged to intermediate/A ‘Levels and 10.20 % to grade VIII and below. There was a significant change between pretest, post-test and follow up readings (Table 1). The frequency of good knowledge (≥ 60%) (Table 1) regarding all components of first aid and basic life support program was significantly higher in the post-intervention and follow up phases than the pre-intervention phase. In student’s situational knowledge about first aid (Figure 1) throughout the interventions, posttest gives the most elevated results in all the categories.
Table 1: Consolidated pre, post and follow up tests scores of knowledge of first aid.
| Sr.
No. |
Questions
Satisfactory Knowledge (60% or above) |
Pretest
Mean±SD 10.80±2.994 n (%) |
χ2-test
(p-value) Pre–Post |
Post Test
Mean ± SD 16.61± 2.627 n (%)
|
χ2-test
(p-value) Post– Follow up |
Follow Up
(After three months) Mean ± SD 15.87± 2.915 n (%) |
χ2-test (p-value) Pre–Follow-up | ||||||
|
|
Which of the followings are the Indications for CPR? | 95 | 66.43 | 2.71
(<0.001)* |
127 | 88.81 | 0.004
(<0.001)* |
106 | 74.12 | 0.399 | |||
|
|
ABC approach in BLS is: | 77 | 53.84 | 0.005 | 97 | 67.83 | 0.35 | 88 | 61.53 | 0.063 | |||
|
|
Initial pulse assessment duration is. | 43 | 30.06 | 1.68
(<0.001)* |
137 | 95.80 | 0.04
(<0.001)* |
119 | 83.21 | 1.04
(<0.001)* |
|||
|
|
The initial BLS steps
for adults are: |
19 | 13.28 | 3.38
(<0.001)* |
46 | 32.16 | 0.45 | 40 | 27.97 | 0.04 | |||
|
|
In one man CPR what is the recommended compression to breathing ratio? | 24 | 16.78 | 2.31
(<0.001)* |
137 | 95.80 | 0.05 | 129 | 90.20 | 8.24
(<0.001)* |
|||
|
|
Compression rate | 32 | 22.37 | 7.76
(<0.001)* |
84 | 58.74 | 0.05 | 75 | 52.44 | 1.86
(<0.001)* |
|||
|
|
When re-assessing the
Victim’s pulse, respiration and chest rise up, we do. |
58 | 40.55 | 1.00 | 123 | 86.01 | 0.28 | 126 | 88.11 | 0.51 | |||
|
|
Where can pulse be easily felt (checked)? | 51 | 35.66 | 1.46
(<0.001)* |
125 | 87.41 | 0.162 | 132 | 92.30 | 9.00
(<0.001)* |
|||
|
|
What is the first thing you should do if you find a collapsed person? | 50 | 34.96 | 9.47
(<0.001)* |
50 | 34.96 | 0.104 | 63 | 44.05 | 2.16
(<0.001)*
|
|||
|
|
What action would you use to open the Person’s airways? | 104 | 72.72 | 2.09
(<0.001)* |
135 | 94.40 | 0.49 | 132 | 92.30 | 6.10
(<0.001)* |
|||
|
|
If the person is not breathing what would you do? | 75 | 52.44 | 0.027 | 89 | 62.23 | 0.008 | 65 | 45.45 | 0.192 | |||
|
|
If the person is breathing what would you do? | 108 | 75.52 | 0.746 | 123 | 86.01 | 0.059 | 79 | 55.24 | 0.091 | |||
|
|
Where in the chest would you press if you were giving chest compressions? |
83 |
58.04 |
4.84
(<0.001)* |
139 | 97.20 | 0.527 | 137 | 95.80 | 1.47
(<0.001)* |
|||
|
|
When should we stop giving CPR?
|
53
|
37.06
|
2.34
(<0.001)* |
79
|
55.24
|
0.062 |
|
45.45 | 0.088 | |||
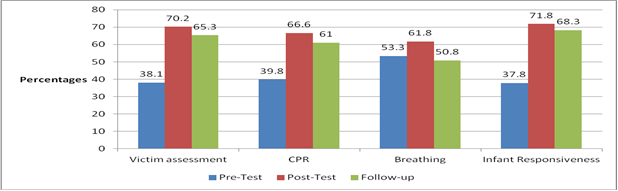
Figure 1: Student’s situational knowledge about first aid throughout the interventions.
In pre-test 126 students out of 143 students got less than 60% (Table 2). In post-test only 40 students got less than the required result. None of the students achieved above 90% in pre, post or follow up but in assessment questions, 3 students got more than 90 % and only 46 students did not get a satisfactory result. In follow up 45 got less than satisfactory result.
Table 2: Grades of Knowledge achieved by the students in first aid training program.
| Test | Grades | ||||
| A*
> 91 % |
A
> 80 – 90.9 % |
B
> 79.9 -70% |
C
> 69.9 – 60% |
F
< 60% |
|
| Pre-Test | 0 | 0 | 1 | 16 | 126 |
| Post-Test | 0 | 10 | 27 | 66 | 40 |
| Follow-Up Test | 0 | 9 | 20 | 53 | 45 |
| Hands on Assessment | 3 | 10 | 39 | 45 | 46 |
Males scored better than the females in pretest (18.75%) but in posttest follow up and assessments females scored extremely better, although again in hands on the boys (93.3 %) fared well (Table 3).
Table 3: Consolidate levels of test among gender, education, and different age groups.
| Parameters | Pre-Test | Post-Test | Follow Up | Hands on Assessment |
| Gender | ||||
| Female (95) | 8.42% | 75.7 % | 62.1% | 88.4 % |
| Male (48) | 18.75 % | 64.58 % | 45.8 % | 95.8 % |
| Levels of Education | ||||
| Secondary (14) | 0 % | 13.9 % | 10.1 % | 13.9 % |
| Matric (78) | 7.5 % | 67.08 % | 51.8 % | 72.1 % |
| Intermediate (51) | 22.4 % | 79.5 % | 65.3 % | 59.1 % |
| Age Groups | ||||
| 13-15 years (53) | 7.5 % | 64.1 % | 54.7 % | 86.7 |
| 16-18 years (90) | 14.4 % | 76.6 % | 57.7 % | 93.3 % |
It is seen that in pre-test students acquired above satisfactory results at intermediate and matric levels respectively whereas none of the students from secondary level (15) got satisfactory result.
In posttest intermediate level, students got highest (79.5%) whereas, matric students got just above satisfactory results (67.08%) and secondary levels getting the lowest (13.9 %). A slight decline of percentages was observed at follow up from Intermediate to secondary levels whereas the hands on practice got maximum 72.1% from matric students (Table 3). In all the levels of intervention higher, the ages better the results.
Pakistan trenchantly expends minimal per unit of the population on health and contains one of the high-rise death rates because of contagious diseases17. A review of 10 studies revealed that laypersons range from 10.7% to 65% attempt giving emergency assistance considering that 83.7% give incorrect first aid 18. The intention was to observe that training of this age group will drive to advancement in their present knowledge. Volunteers from a tertiary care hospital aged 13-18 years with a mean age of 15.29±1.24 years were chosen as this age cohort has remarkable keenness and zests to inculcate and obtain knowledge and to brighten their skills by hands-on rehearse19. In a study of Zagazig University, the preparatory school children aged 11-16 years got significant results in pre-post and pre-follow up (p<0.001) in basic life support and choking16.
In another study, it was seen that concept of CPR training can be conveyed very effectively to schoolchildren20. A study in primary and secondary schools bystanders CPR (BCPR) achieved positive results before and after the training21. Results of pre, post and follow-up combined scores conclude significant changes. The standard knowledge of BLS had a mean value of 10.8± 2.99. Whereas an analogous study observed very low, BLS and choking baseline result in school students22. Many different Medical school’s studies also showed a low level of first aid knowledge23.
In post-test, the acquired results were above 60 % where as they dropped in the follow up (3 months after the intervention). These results were consistent with another study where the intervention was given to school health advisors in Qassim province KSA (Kingdom of Saudi Arabia) in which it showed significantly higher results in post-intervention and follow up phases19. Masih et al. showed low pre-test, post-test knowledge mean scores as 27.32 ±5.73 and 34.76 ± 4.35 respectively23. In the current study it was observed that in pretest males fared better than females but the other two times namely post-test and follow up girls got better results. While in hands on practice boys scored more than the girls. An Indian study in undergraduate students showed contrasting results that 11.5% of males and 15.4% of females had a satisfactory level of knowledge on first aid measures24.
This study included different levels of education specifically secondary, matric and intermediate but none of the students got a satisfactory result from the secondary level in Pre-test, whereas intermediate was better than matric students. The Post-test and follow up results of intermediate students were better than the matric and secondary students. Hands on practice had better results from matric students, the second was intermediate students, and secondary student’s scores were the least. The results were similar to the Student’s knowledge as documented by another study23.
A comparison was done between 13-15, 16-18 years old in this study and it was seen that at all the levels i.e., pre, post-test, follow up, and assessment higher the age better the results were achieved. This is consistent with the study on health advisors that showed with increasing age and education level that the trainees achieve better scores21. The strength of the study was that it is an interventional study and since the participants were chosen from an already running volunteer program, the budget was immensely reduced. Limitations were time and budget constraints due to which randomized control trial could not be executed which would have been an ideal study design otherwise. The participants selected from schools would have given results that are more generalizable but selection bias was there, as permissions were not allowed, all the aspects of first aid could not be explored due to lack of time and budget.
Knowledge and skills about FA may be integrated and CPR skills may be focused and improved. Evidence based studies should be conducted in schools at large to assess knowledge and attitudes towards FA/CPR in society. Incidences and consequences of school-age child injuries may be assessed by further researches. The finding of the research strongly recommends that these training may be made part of the school curriculum.
First aid training delivered to the volunteers was very effective and more training may be conducted at larger scales in schools. Adding first aid training in the curriculum may act as fundamental for present and future national emergencies as well as normal control.
The authors would like to acknowledge their teachers, families, unit heads and students for being an inspiration.
The authors declare no conflict of interest.
Ethical Approval was obtained from the hospital administration to conduct the research and intervention. The proposal was submitted to Institutional Review Board of APPNA Institute of Public Health with the IRB reference number: JSMU/IRB/2017/-89.
Informed consent was obtained from parents of all participating students’ (as the participants are less than 18 years) and confidentiality was maintained.
MO developed the concept, wrote the introduction and also contributed in methodology development and helped in data collection. SM helped in development of the concept and writing of methodology and results. FE did data analysis and wrote the results. SS helped in data analysis as well. FA wrote results and discussion while FZ helped in discussion and abstract writing. MT helped in introduction writing too. BA did data analysis, results formulation and results writing.
- De Buck E, Laermans J, Vanhove AC, Dockx K, Vandekerckhove P, Geduld H. An educational pathway and teaching materials for first aid training of children in sub-Saharan Africa based on the best available evidence. BMC Public Health. 2020; 20:1-6.
- Panchal AR, Berg KM, Hirsch KG, Kudenchuk PJ, Del Rios M, Cabañas JG, et al. 2019 American Heart Association focused update on advanced cardiovascular life support: use of advanced airways, vasopressors, and extracorporeal cardiopulmonary resuscitation during cardiac arrest: an update to the American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2019;140(24):e881-e894.
- Al-Musa HM, Bharti RK, Alsamghan AS, Asiri M, Alqahtani MS, Al-qahtani D, et al. Knowledge of first aid skills among medical students in King Khalid University, Abha, Saudi Arabia. People’s J Sci Res. 2017;10(1):1-6.
- Ganfure G, Ameya G, Tamirat A, Lencha B, Bikila D. First aid knowledge, attitude, practice, and associated factors among kindergarten teachers of Lideta sub-city Addis Ababa, Ethiopia. PloS one. 2018;13(3):e0194263:1-15.
- Al-Hajj S, El Bcheraoui C, Daoud F, Khalil I, Moradi-Lakeh M, Abu-Raddad LJ, et al. Child and adolescent injury burden in the eastern mediterranean region: Findings from the Global Burden of Disease 1990-2017. BMC Public Health. 2020;20:1-10.
- Chokotho L, Mulwafu W, Singini I, Njalale Y, Maliwichi-Senganimalunje L, Jacobsen KH. First responders and prehospital care for road traffic injuries in Malawi. Prehosp Disaster Med. 2017;32(1):14-19.
- Başer M, Çoban S, Taşci S, Sungur G, Bayat M. Evaluating first-aid knowledge and attitudes of a sample of Turkish primary school teachers. J Emerg Nurs. 2007;33(5):428-432.
- Afifi RM, Zaytou SS, El Raggal AA, Qulali A, Ayoub HA. Involvement of male youth into accidents in upper Egypt: Pattern and risk analysis. Health. 2015;7(08):965-974.
- Peterson TD, Noland S, Russell DW, Paradise NF. Bystander trauma care training in Iowa. Prehosp Emerg Care. 1999;3(3):225-230.
- Olumide AO, Asuzu MC, Kale OO. Effect of first aid education on first aid knowledge and skills of commercial drivers in South West Nigeria. Prehosp Disaster Med. 2015;30(6):579-585.
- Wilks J, Kanasa H, Pendergast D, Clark K. Emergency response readiness for primary school children. Aust Health Rev. 2016;40(4):357-363.
- Asim M, Ahmad B, Salam M. Household’s willingness to pay for solid waste management, parks maintenance and horticulture services (selected areas of Karachi-case in point). Glob Manag J Acad Corp Stud. 2016;6(2): 116-128.
- Khan A, Shaikh S, Shuaib F, Sattar A, Samani SA, Shabbir Q, et al. Knowledge attitude and practices of undergraduate students regarding first aid measures. J Pak Med Assoc. 2010;60(1):68-72.
- Mohammed AA. The influence of training program on knowledge and practices of preparatory schools’ children related to the selected first aid. Am J Nurs. 2018;6(4):158-163.
- Deekshitha P, Dhivya K, Pravallika S, Lavanya D, Kesini M. Evaluation of knowledge, attitude and practice on first aid measures among students. Indian J Public Health Res Develop. 2018;9(10):50-56.
- Wafik W, Tork H. Effectiveness of a first‐aid intervention program applied by undergraduate nursing students to preparatory school children. Nurs Health Sci. 2014;16(1):112-118.
- World Health Organization. World health statistics 2010 [Internet]. World Health Organization, 2010 [cited 2020 Sep 16]. Available from: https://www.who.int/whosis/whostat/2010/en/
- Tannvik TD, Bakke HK, Wisborg T. A systematic literature review on first aid provided by laypeople to trauma victims. Acta Anaesthesiol Scand. 2012;56(10):1222-1227.
- Campbell S. Supporting mandatory first aid training in primary schools. Nurs Stand. 2012;27(6):35-39.
- Jones I, Whitfield R, Colquhoun M, Chamberlain D, Vetter N, Newcombe R. At what age can schoolchildren provide effective chest compressions? An observational study from the Heartstart UK schools training programme. BMJ. 2007;334(7605):1201-1203.
- Behairy AS, Al-Batanony MA. Effectiveness of first-aid and basic life support intervention program on school health advisors. J Health Med Nurs. 2015;24:136-144.
- Sharma S. Knowledge of first aid among undergraduate students of KMC, Mangalore. New Indian J Surg. 2011;2:p.401.
- Masih S, Sharma RK, Kumar A. Knowledge and practice of primary school teachers about first aid management of selected minor injuries among children. International Journal of Medicine and Public Health. 2014;4(4): 458-462.
- Kanstad BK, Nilsen SA, Fredriksen K. CPR knowledge and attitude to performing bystander CPR among secondary school students in Norway. Resusc. 2011;82(8):1053-1059.
This is an open-access article distributed under the terms of the CreativeCommons Attribution License (CC BY) 4.0 https://creativecommons.org/licenses/by/4.0/