By Hafiz Muhammad Aamir Riaz1, Sara Qureshi1, Qudsia Iqbal2, Insha Ajmal Malik3, Muhammad Waseem Ullah Khan4, Momina Akram1
- Department of Prosthodontics, de’Montmorency College of Dentistry, Lahore, Punjab, Pakistan.
- Department of Prosthodontics, Rawal Institute of Health Sciences, Islamabad, Punjab, Pakistan.
- Dentist.
- Department of Prosthodontics, Dental Institute, Punjab Medical College, Faisalabad, Medical University, Faisalabad, Punjab, Pakistan.
DOI: https://doi.org/10.36283/PJMD12-2/010
How to cite: Riaz HMA, Qureshi S, Iqbal Q, Malik IA, Khan MWU, Akram M. The Shortened Dental Arch Concept: Awareness and Opinion of Dentists in Lahore, Pakistan. Pak J Med Dent. 2022;12(2): 56-61. doi: 10.36283/PJMD12-2/010
Background: Dental arches maintain the chewing function when a set of four symmetrical occluding units are present. This study aimed to evaluate the understanding and acknowledgment of the shortened dental arch (SDA) concept and its clinical applicability by the dentists of Lahore, Pakistan; and interpret dentists’ appraisal regarding the patients’ responses to SDA application concerning chewing ability, oral comfort and dentofacial appearance.
Methods: A self-administered questionnaire was voluntarily filled out by 250 anonymous dentists in Lahore, Pakistan. Data were statistically analyzed using SPSS software version 25. This descriptive cross-sectional study was conducted in Lahore, Pakistan from December 2021 to June 2022 for a period. Data collected were statistically analyzed using SPSS software version 25. Mean standard deviation was given for age, clinical experience and the average number of patients seen monthly. p-value ≤ 0.01 was considered statistically significant.
Results: Approximately half of the informants (51.6%) were unaware of the SDA concept. A significant difference existed between the clinical experience of dentists and their cognizance of the shortened dental arch notion. Only 32.6% of the ‘aware’ dentists had clinically implemented the SDA concept in the past year. Chewing function and oral comfort of patients with SDA was presumed to be fairly acceptable by 40.8% (102) and 46.4% (116) of the dentists respectively.
Conclusion: The majority of the responding dentists had a paucity of knowledge regarding the SDA concept. Despite this, a significant proportion of dentists regarded the chewing function, oral comfort and dental appearance to be fairly satisfying in individuals with shortened dental arches.
Keywords: Awareness, Chewing Function, Oral Comfort, Shortened Dental Arch (SDA).
Arnd Kayser, the first prosthodontist, to meaningfully construe the idea of the shortened dental arch in 1981 for a dentition that has a minimum of four congruous occluding units (one unit conforms to a set of two occluding premolars; whereas a set of two occluding molars is equivalent to two units) 1. This treatment approach correlates with the adaptive capacity of older individuals and therefore meets their requirements of oral function to an acceptable level thereby reducing the cost of treatment2.
The conceptualization of shortened dental arch has faced sheer criticism from many traditional clinicians. It has been regarded that the unfortunate loss of molar teeth is accompanied by a compromised masticatory function and a relative risk factor for complications in TMJ3. SDA has also been suggested to be associated with occlusal instability which occurs due to tooth migration4.
However, the controversial opinions regarding the influence of shortened dental arch on masticatory function have frequently skewed from a negative towards a positive approach. Research validates that shortened dental arches successfully maintain the chewing function when a set of four symmetrical occluding units are present5. The minor occlusal changes that occur concerning shortened dental arches are therefore self-limiting and have sufficient adaptive capacity. WHO guidelines that have been published in 1992 consider the concept of the shortened dental arch as a viable alternative in certain clinical conditions where there are limited restorative possibilities for posterior teeth and patients experiencing financial constraints6. Moreover, there is no conclusive evidence that depicts a positive correlation between a shortened dental arch and craniomandibular dysfunction7. Missing posterior teeth are replaced mainly for the patient’s desire or as a conscious decision by a dentist for the preservation of oral function. Conventional prosthodontic rehabilitation strategy for the missing posterior dentition has long been removable partial dentures (RPDs). However, the use of free-end saddle removable partial dentures is significantly associated with an increased risk of cumulating plaque, tooth decay, periodontitis and residual ridge resorption8. Since RPDs are a significant contributing factor to root surface caries, SDA is considered to be a viable treatment approach for elderly persons with inadequate oral hygiene9.
Cantilever resin-bonded fixed dental prosthesis is a well-precedented treatment option to restore the shortened dental arch status in patients who have less than four occlusal units10. Due to the high biological cost associated with RPDs, cantilever resin-bonded fixed dental prosthesis is a more acceptable alternative option for the replacement of distal extension-free end saddles.
Single-tooth implants are considered to be a viable treatment modality with promising results for the replacement of missing posterior teeth11. However various complications have been reported that significantly affect the success and survival rates of implant-supported prostheses. These include peri-implantitis, prosthesis fracture and marginal bone loss12.
The restoration of the missing posterior dentition by distal extension removable dentures, cantilever resin-bonded bridges or fixed implant prosthesis are all considered to be overtreatment for older adults with shortened dental arch status. Although the concept of a shortened dental arch has received widespread acceptance, it is still not practiced by the majority of dentists. Hence, there is a need to evaluate the discrepancy between the dentist’s attitude toward SDA and the patient’s preference for alternative treatment options to restore missing posterior teeth.
The present study aimed to assess the knowledge, perception and clinical applicability of SDA by the dentists in Lahore, Pakistan; and evaluate dentists’ appraisal regarding the patients’ responses to SDA application in terms of chewing efficiency, oral comfort and dentofacial appearance.
This was a cross-sectional study conducted on n=250 dentists. A self-administered questionnaire was voluntarily filled by a random sample of anonymous dentists in Lahore, Pakistan from December 2021 to June 2022 for a period The questionnaire had 25 sequentially arranged questions. The first part was about the demographic details of dentists and their knowledge about the shortened dental arch. The second part involved questions regarding the dentists’ opinions and the clinical applicability of this concept. The last part of the questionnaire had questions concerning dentists’ assessment of patients’ responses and their perceived benefits when the concept of the shortened dental arch was clinically implemented. Ethical approval was taken from the ethical review board of de’Montmorency College of Dentistry, Lahore. Data collected were statistically analyzed using SPSS software version 25. Mean standard deviation was given for age, clinical experience and the average number of patients seen monthly. p ≤ 0.01 was considered statistically significant.
The n=250 respondents had a mean age of 28.82±7.69 years. The mean clinical experience of the respondents was 4.03±4.57 years with an average of 109±62.25 patients seen in a month. The majority of the respondents (64.8%) had only a basic dental degree with no postgraduate qualification.
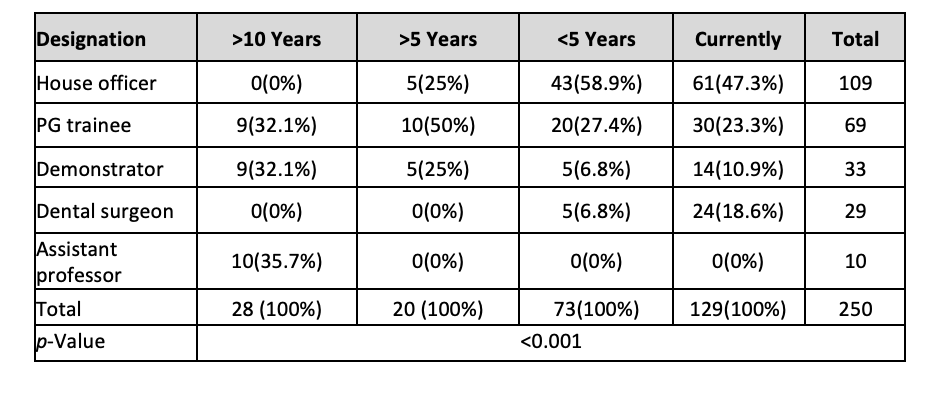
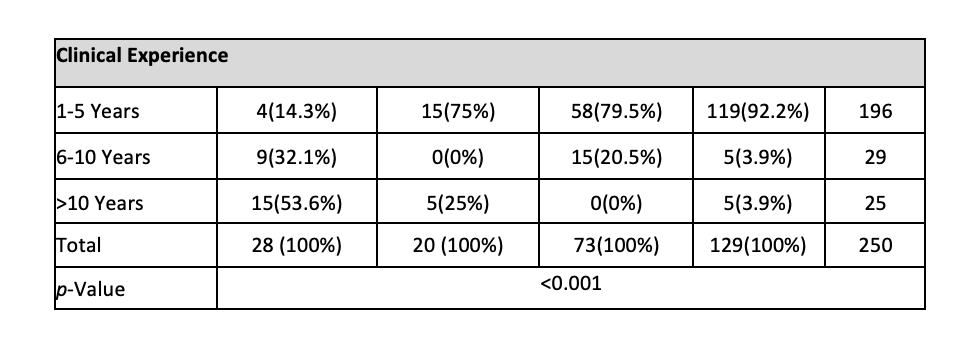
A substantial proportion of dentists were unaware of the concept of the shortened dental arch (51.6%), however, only a small percentage (11.2%) of dentists had known this concept more than 10 years ago. Out of the ‘aware’ dentists, 32.6% had practically applied this concept to their patients in the past year. Only 28(11.2%) dentists reported that they have applied this treatment option to ≥ 50% of the patients, while 35(14%) reported that they have applied it to their <10% of the patients. It has been found that dentists who were designated as assistant professors (AP) had more awareness of the SDA concept. There was a positive correlation between the knowledge of the SDA concept and years of clinical experience of a dentist. Those who had 6-10 years or greater than 10 years of experience in clinical dentistry had a better understanding of the SDA concept than those with less than 5 years of experience. The distinction in the awareness of the SDA concept about the designation and clinical experience was statistically significant (p <0.001) as delineated in Table 1.
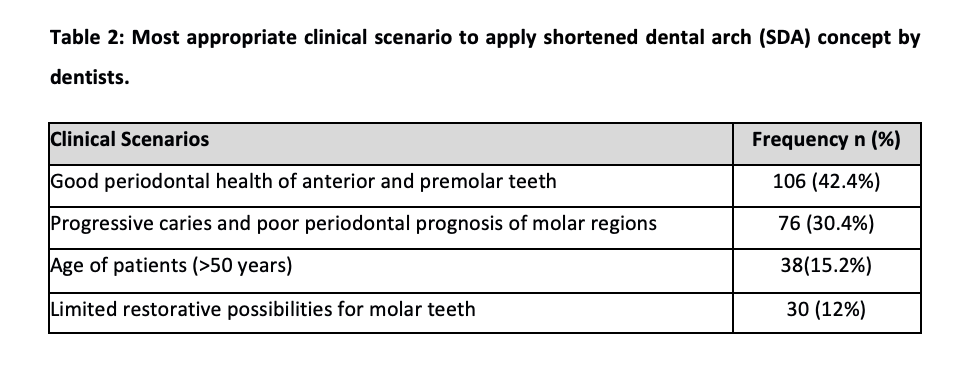
Dentists’ opinion regarding the implementation of the SDA concept in the most desirable clinical scenario was also taken into account. It was evinced that 42.4% of the dentists intended to apply this concept to a clinical scenario where the patient has an above-average periodontal prognosis of anterior and premolar teeth as shown in Table 2. Moreover, the most common reason given by dentists (58.4%) to replace missing molars was to maximize the masticatory function in elderly patients.
Dentists who were knowledgeable of this concept ascertained the response of patients when SDA was given as a treatment option to them. Thus, 25.6% of the dentists had a viewpoint that patients initially rejected the SDA treatment option, however, they later accepted it after a thorough explanation by the dentist.
Dentists’ opinion regarding the chewing function, oral comfort and dental appearance of the patients with the shortened dental arch was taken into account as shown in Figure 1. Regarding the assessment of chewing function in patients with shortened dental arch, 40.8% (102) dentists found it to be fairly satisfying whereas 21.2% (53) considered it to be poor hence severely compromising the masticatory efficiency. 46.4% (116) dentists thought that oral comfort was fairly acceptable. The dental appearance of patients with the shortened dental arch was categorized as good by 30.8% (77) dentists, however, 15.6% of the dentists regarded the dental appearance as poor and clinically unacceptable.

The study found 32.6% of the ‘aware’ dentists had clinically implemented the SDA concept in the past year. Abuzar et al. studied the awareness of the shortened dental arch among the dentists of Australia2. He concluded that almost 61% of the respondents were aware of the SDA concept. However, 78.4% of dentists had an optimistic opinion regarding the efficacious clinical applicability of the SDA notion. Shortened Dental Arch has long been introduced in dentistry. Although it is based on circumstantial evidence still it has not achieved the deserved affirmation by many dentists around the world. The SDA concept offers multifold advantages which outweigh the merits of replacing missing posterior teeth with different treatment modalities. Another cross-sectional survey was conducted in Jordan which reveals that 82.1% of the Jordanian dentists were aware of the SDA concept and dentists with fewer years of clinical experience had better awareness of it than those with more years of experience13.
However, our study reported dissimilar findings because the majority of the dentists in Lahore, Pakistan was unaware of the SDA concept and only those dentists who had more clinical experience expressed better awareness of this concept. A study conducted by Kasim et al.14 showed that 86.9% of Malaysian government dentists were familiar with the concept of SDA. Moreover, an appreciable percentage of the dentists who had ≤5 years of clinical experience acknowledged SDA as a simplified treatment approach when compared with the dentists having >5 years of clinical experience. A questionnaire-based study was employed to determine the awareness of the SDA concept among the dentists of the United Arab Emirates15. The conclusions drawn from it revealed that 65.8% of the dentists in UAE were aware of the SDA concept however the majority of the dentists were reluctant to apply it in clinical practice due to the possible risks of abutment drifting and temporomandibular disorders.
Many foregoing studies conclude that shortened dental arches which involve anterior and posterior premolar teeth can efficiently fulfill the demands of a functional dentition thereby providing adequate oral comfort and improved oral hygiene with possibly reduced treatment charges. The studies conducted on the chewing efficiency of individuals with shortened dental arches infer that the presence of sound premolars along with a single pair of occluding molars is deemed enough for adequate masticatory performance16. However masticatory efficiency will only become ineffectual when there are less than 20 symmetrically distributed teeth in the oral cavity.17 Despite this, the decision to replace the missing molar teeth is strongly influenced by the subjective evaluation which varies from patient to patient. Moreover, financial constraints also out-turn the choice of treatment. A cross-sectional survey was conducted by Abu-Awwad et al.13 which revealed that Jordanian dentists considered the replacement of missing molars necessary to ameliorate the masticatory efficiency of patients. This was following the findings of our study where dentists intended to replace missing molars to maximize mastication, especially in older patients. Sarita et al.18 in their study evaluated the attitude of dentists in Tanzania regarding the clinical applicability of the SDA concept. The results show that 71% of the responding dentists considered the chewing efficacy of the individuals with shortened dental arches to be satisfactory or acceptable. Furthermore, only 48% of the dentists presumed acceptable oral comfort in an individual with a shortened dental arch.
Contemporary research depicts that mastication is significantly improved after the restoration of shortened dental arches with removable partial dentures19. However, it negates the results of previous studies where the restoration of free-end saddles with removable partial dentures had no discernible improvement in masticatory function20. A randomized controlled trial was conducted for 10 years to compare oral health in individuals with shortened dental arches and those with replaced missing molars by removable partial dentures. No remarkable difference was noted in the two treatment modalities21. Due to these conflicting reviews, many dentists are still hesitant in the clinical application of this concept while others are not even acquainted with it.
This cross-sectional survey determines the understanding of shortened dental arch by the dentists of Lahore, Pakistan and their preference to choose it as an appropriate treatment alternative among preferable individuals. Moreover, it describes the dentist’s assessment regarding the response of the patient to this treatment modality. Confoundingly, almost half of the informants (51.6%) were unaware of the SDA concept and a considerable percentage of dentists (66.4%) had not clinically applied this concept in the past year. These results controvert the findings of previous studies stated above. It can be deduced that a significant proportion of dentists regarded the application of this concept in patients who had a good periodontal prognosis of anterior teeth and premolars. According to this survey, a significant proportion of dentists perceived that the chewing function, oral comfort and dental appearance are fairly satisfying in individuals with a shortened dental arch. However, a small percentage of dentists had a pessimistic opinion regarding the usefulness of this concept. 21.2% of dentists considered the chewing function of individuals with SDA to be notably impaired and graded it as poor.
The majority of dentists lacked knowledge of the shortened dental arch concept. Those who were aware of it had certain reservations regarding it. Even if they encounter an appropriate clinical scenario for its application, they tend to be ambivalent in assessing its relative pros and cons. However, many dentists thought that SDA patients had a fairly acceptable oral function and dental appearance.
The authors would like to acknowledge the institution for its support throughout the study.
The authors declared no conflict of interest.
This study has been approved by the ethics review committee of the institution.
Consent of the participants was taken before recruitment in the study.
All the authors equally contributed in the research study.
Kanno T, Carlsson GE. A review of the shortened dental arch concept focusing on the work by the Käyser/Nijmegen group. J Oral Rehabil. 2006;33(11):850-862. doi: 10.1111/j.1365-2842.2006.01625.x
- Abuzar M, Humplik A, Shahim N. The shortened dental arch concept: awareness and opinion of dentists in Victoria, Australia. Aust Dent J. 2015;60(3):294-300. doi: 10.1111/adj.12245
- Tallents RH, Macher DJ, Kyrkanides S, Katzberg RW, Moss ME. Prevalence of missing posterior teeth and intra articular temporomandibular disorders. J Prosthet Dent. 2002;87(1):45-50. doi: 10.1067/mpr.2002.121487
- Witter DJ, Creugers NHJ, Kreulen CM, de Haan AFJ. Occlusal stability in shortened dental arches. J Dent Res. 2001;80(2):432-436. doi: 10.1177/00220345010800020601
- Armellini D, von Fraunhofer JA. The shortened dental arch: A review of the literature. J Prosthet Dent. 2004;92(6):531-535. doi: 10.1016/j.prosdent.2004.08.013
- WHO Expert Committee on Recent Advances in Oral Health, Organization WH. Recent advances in oral health : report of a WHO expert committee [meeting held in Geneva from 3 to 9 December 1991] [Internet]. apps.who.int. 1992. Available from: https://apps.who.int/iris/handle/10665/39644
- Witter DJ, Haan AFJ, Käyser AF, Rossum GMJM. A 6-year follow-up study of oral function in shortened dental arches. Part II: Craniomandibular dysfunction and oral comfort. J Oral Rehabil. 1994;21(4):353-366.
- Wöstmann B, Budtz-Jørgensen E, Jepson N, Mushimoto E, Palmqvist S, Sofou A, et al. Indications for removable partial dentures: a literature review. Int J Prosthodont. 2005;18(2):139-145.
- Jepson NJA, Moynihan PJ, Kelly PJ, Watson GW, Thomason JM. Caries incidence following restoration of shortened lower dental arches in a randomized controlled trial. Br Dent J. 2001;191(3):140-144. doi: 10.1038/sj.bdj.4801122
- Thomason JM, Moynihan PJ, Steen N, Jepson NJA. Time to survival for the restoration of the shortened lower dental arch. J Dent Res. 2007;86(7):646-650. doi: 10.1177/15440591070860071
- Misch CE, Misch-Dietsh F, Silc J, Barboza E, Cianciola LJ, Kazor C. Posterior implant single-tooth replacement and status of adjacent teeth during a 10-year period: a retrospective report. J Periodontol. 2008;79(12):2378-2382. doi: 10.1902/jop.2008.080188
- Goodacre CJ, Bernal G, Rungcharassaeng K, Kan JYK. Clinical complications with implants and implant prostheses. J Prosthet Dent. 2003;90(2):121-132. doi: 10.1016/S0022-3913(03)00212-9
- Abu-Awwad M, Amarin R, Khouli F, Shaban S, AlTarawneh S. Dentists’ Attitudes in Jordan towards the Shortened Dental Arch Concept: A Cross-Sectional Study. Int J Dent. 2019;2019:1-6. doi: 10.1155/2019/4163851
- Kasim SKM, Razak IA, Yusof ZYM. Knowledge, perceptions and clinical application of the shortened dental arch concept among Malaysian government dentists. Int Dent J. 2018;68(1):31-38. doi: 10.1111/idj.12325
- AlHmoudi H, Khamis AH, Elbishari H, Amir-Rad F. The Shortened Dental Arch Concept: Awareness, Knowledge, and Practice of Dentists in Dubai and the Northern Emirates, United Arab Emirates. Int J Dent. 2022;2022:1-7. doi: 10.1155/2022/6018650
- Rosenoer LM, Sheiham A. Dental impacts on daily life and satisfaction with teeth in relation to dental status in adults. J Oral Rehabil. 1995;22(7):469-480. doi: 10.1111/j.1365-2842.1995.tb01191.x
- Omo JO, Sede MA, Esan TA. Masticatory efficiency of shortened dental arch subjects with removable partial denture: A comparative study. Niger J Clin Pract. 2017 ;20(4):459-463. doi: 10.4103/1119-3077.181363
- Sarita PTN, Witter DJ, Kreulen CM, Creugers NHJ. The shortened dental arch concept – attitudes of dentists in Tanzania. Community Dent Oral Epidemiol. 2003;31(2):111-115. doi: 10.1034/j.1600-0528.2003.00018.x
- Sarita PTN, Witter DJ, Kreulen CM, Van’t Hof MA, Creugers NHJ. Chewing ability of subjects with shortened dental arches. Community Dent Oral Epidemiol. 2003;31(5):328-334. doi: 10.1034/j.1600-0528.2003.t01-1-00011.x
- Witter DJ, Elteren P, Käyser AF, Rossum MJM. The effect of removable partial dentures on the oral function in shortened dental arches. J Oral Rehabil. 1989;16(1):27-33. doi: 10.1111/j.1365-2842.1989.tb01314.x
- Reissmann DR, Wolfart S, John MT, Marré B, Walter M, Kern M, et al. Impact of shortened dental arch on oral health-related quality of life over a period of 10 years — A randomized controlled trial. J Dent. 2019;80:55-62. doi: 10.1016/j.jdent.2018.10.006
This is an open-access article distributed under the terms of the CreativeCommons Attribution License (CC BY) 4.0 https://creativecommons.org/licenses/by/4.0/