By Aeman Ali1, Afifa Razi1, Atif Butt2, Saima Sameer Qureshi3, Nosheen Nazir1, Amina Ali1
- Department of Oral Medicine and Diagnosis, Ziauddin College of Dentistry, Karachi, Pakistan.
- Oral and Maxillofacial Surgery, Ziauddin College of Dentistry, Karachi, Pakistan.
- Department of Periodontology, Ziauddin College of Dentistry, Karachi, Pakistan.
DOI: https://doi.org/10.36283/PJMD12-2/006
How to cite: Ali A, Razi A, Butt A, Qureshi SS, Nazir N, Ali A. Frequency of Distal Caries of 2nd Molar with Mesio-Angular Impaction in Subset of Karachi Population. Pak J Med Dent. 2022;12(2): 29-35. doi: 10.36283/PJMD12-2/006
Background: The oral cavity has four 3rd molars, commonly termed wisdom teeth. These molars may erupt in an appropriate anatomical place and become functional, or they may erupt partly or non-functionally, in which case they are known to as impacted. Therefore, the study aimed to measure the frequency of distal caries of 2nd molars in the presence of mesio-angular impacted 3rd molars and its association with the other type of impactions among patients.
Methods: It was a retrospective cross-sectional study done at the Oral Medicine and Diagnosis Department of Ziauddin University Hospital in Karachi, Pakistan. The study comprised 201 radiographs of individuals aged 21 to 45 years, of both genders, who visited a dental OPD between 2017 and 2020 and had erupted 2nd molar teeth and impacted 3rd molar teeth in the same quadrant. Patients with inadequate diagnostic quality and distortion on their OPGs were excluded from the research. All collected data were analyzed using SPSS 25.
Results: The frequency of distal caries of 2nd molars was observed to be 122 (60.7%). A total of 103 of the 201 subjects had mesio-angular impaction causing caries in the 2nd molars (84.4%). There was a statistically significant relationship between impaction type and distal caries of 2nd molars (p=0.001). The type of impaction also showed a significant association with gender (p=0.048).
Conclusion: Higher frequency of distal caries of 2nd molars in the presence of mesio-angular impacted 3rd molars was observed. This was also significantly associated with the type of impaction (p<0.001) and gender (p=0.048).
Keywords: Dental Caries, Third Molar, Wisdom Tooth.
The oral cavity has four 3rd molars, commonly termed wisdom teeth, which are the last of the 32 teeth to erupt in the mouth. The age at which eruptions occur varies greatly, and they can occur as early as 17 to 24 years old or as late as the 3rd or 5th decade of life1,2. These molars may erupt into the appropriate anatomical place and become functional, or they may erupt partly or non-functionally, in which case they are known to as impacted. The risk of impaction is significantly higher in the mandibular 3rd molar, and it is influenced by gender, age, ethnicity, lack of space, eruption and growth direction, and growth process2-4.
Due to a lack of space or barrier, third molars are often held back during an eruption, making this area less accessible for oral hygiene practices5,6. If they are enclosed or embedded, they gather plaque, increasing the odds of infection in the posterior molar region7,8. Hence, impacted 3rd molars may cause periodontal disease, pain, pericoronitis, tumor, cyst formation, distal caries, dental crowding, and angle fracture7,8.
One of the most common complications related to the topographic status of the impacted mandibular 3rd molar is distal caries of the mandibular 2nd molar and accounted for 0.5% to 20% 8-12. A recent study by Altiparmak et al. reported, 38.7% of dental caries in 2nd molars developed due to neighboring impacted mandibular 3rd molars13. In a study conducted by Srivastava et al. 38% of the patients had distal caries among 2nd mandibular molars14. According to Ashar et al. prevalence of distal caries was observed to be 40.8% in the mandibular molar 2nd molar caused by impacted third molars15. Another study conducted by Rauf et al. revealed that mesio-angular impaction of the 3rd molar was the commonest impaction which caused distal caries in the neighboring 2nd molars16. Whereas, Raheem et al. found that most distal caries in the 2nd molar were due to the horizontal position of the 3rd molar17.
Evidence suggests that removal of 3rd molars at an early stage can prevent distal caries in 2nd molars, halting tooth loss15,16. There is a paucity of information on its prevalence among Karachi residents. Thus, the goal of this research was to measure the frequency of distal caries of 2nd molars in the presence of impacted 3rd molars and its association with a type of impaction among patients presented at a tertiary care hospital in Karachi, Pakistan.
It was retrospective cross-sectional research conducted at the Oral Medicine and Diagnosis Department of the Ziauddin University Hospital in Karachi, Pakistan. With the prevalence of distal caries set at 40.8% 15, the margin of error set at 6.8%, and the confidence level set at 95%, the sample size of 201 was computed using the Open Epi sample size online calculator. The study comprised 201 radiographs of individuals aged 21 to 45 years, either male or female, who visited a dental OPD between 2017 and 2020 and had erupted 2nd molar teeth and impacted 3rd molar teeth in the same quadrant. The OPGs with inadequate diagnostic quality and distortion were excluded from the research. A non-random convenience sampling approach was used.
The research proposal was submitted and approved by the ethical review board of Ziauddin University Hospital, Karachi, Pakistan. The ethical review board approved the research ERC no. 3590421AAOM. Each radiograph was assessed by postgraduate students from the Ziauddin University Hospital’s Oral Medicine and Diagnosis Department in Karachi, Pakistan. Radiographs with impacted 3rd molars were included in the study. The incidence of distal caries in the mandibular 2nd molars was examined using radiographs with impacted 3rd molar teeth. The gender, age, and kind of impaction of these OPGs were investigated.
The data was analyzed using SPSS version 23. For age in years, the mean and standard deviation were calculated. For age groups (21 to 29 years, 30 to 39 years and 40 to 49 years), gender (male and female), kind of impaction (mesio-angular, distoangular, vertical, and horizontal), and presence of distal caries (yes or no), the frequency and percentage were computed. The association between distal caries and age, gender, and type of impaction was investigated using the Chi-square/Fisher exact test. Association between type of impaction with age and gender was also assessed using Chi-square/Fisher exact test. A p-value<0.05 was considered statistically significant. Effect modifiers such as age, and gender were addressed through stratification and post-stratification chi-square was applied.
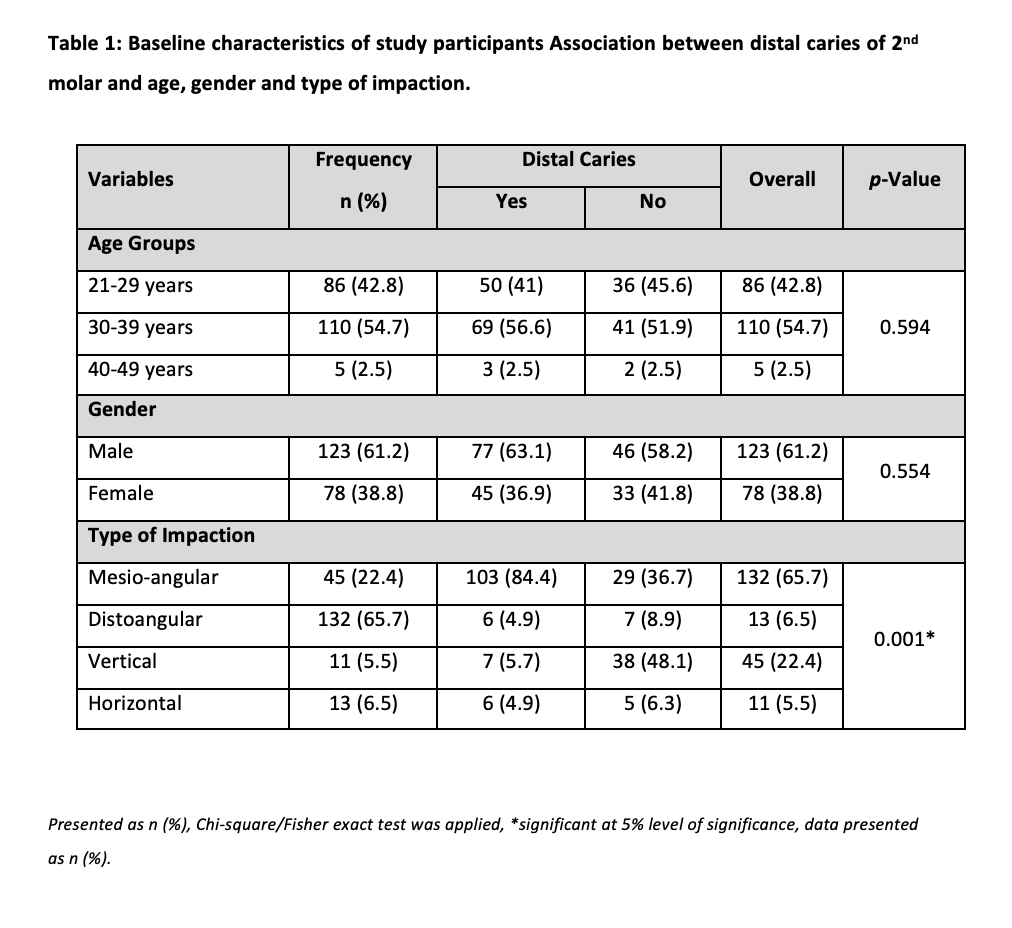
The respondents’ mean age was 30.89±5.39 years, with a range of 21 to 42 years (Figure 1). There were 123 (61.2%) men and 78 (38.8%) females among the 200 participants. More than half of the participants were between the ages of 30 and 39 (54.7%), 42.8% were of age 21-29 years and only 2.5% were of age 40-49 years. The mesio-angular dimension (65.7%) and vertical dimension (22.4%) of the 3rd molar teeth were commonly affected (Table 1). A total of 200 patients with impacted 3rd molar teeth were evaluated, and among them, the frequency of distal caries of 2nd molars was observed to be 122 (60.7%) (Figure 2).

The highest frequency of distal caries of 2nd molars was observed in the age bracket 30-39 years (56.6%), however, the relationship between distal caries and age groups was statistically insignificant (p=0.594). As compared to females, the frequency of distal caries of 2nd molar was more in males, but the relationship between gender and distal caries was statistically insignificant (p=0.554). A total of 103 of the 200 subjects had mesio-angular impaction causing caries in the 2nd molars (84.4%). Whereas, horizontal and distoangular impaction caused the least distal caries in the 2nd molars (4.9% each). There was a statistically significant relationship between impaction type and distal caries of 2nd molars (p=0.001) (Table 1).
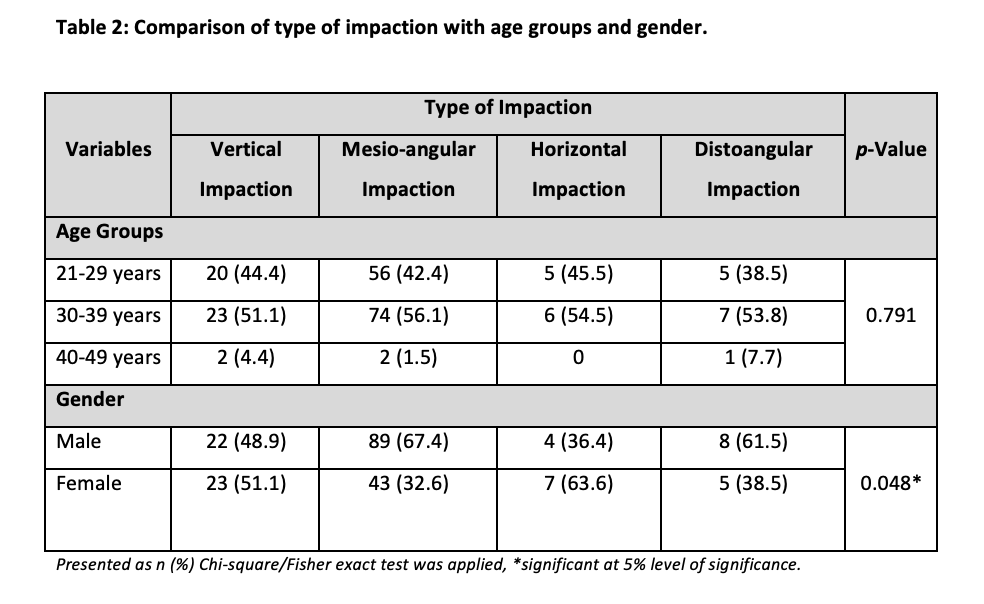
The highest frequency of vertical impaction, mesio-angular impaction, horizontal impaction and disto-angular impaction was observed in the age range 30-39 years, however, the relationship between the type of impaction and age groups was statistically insignificant (p=0.791). As compared to females, the frequency of mesio-angular impaction and disto-angular impaction was more in males, whereas the frequency of vertical impaction and horizontal impaction was higher in females than males. The relationship between the type of impaction and gender was statistically significant (p=0.048) (Table 2).
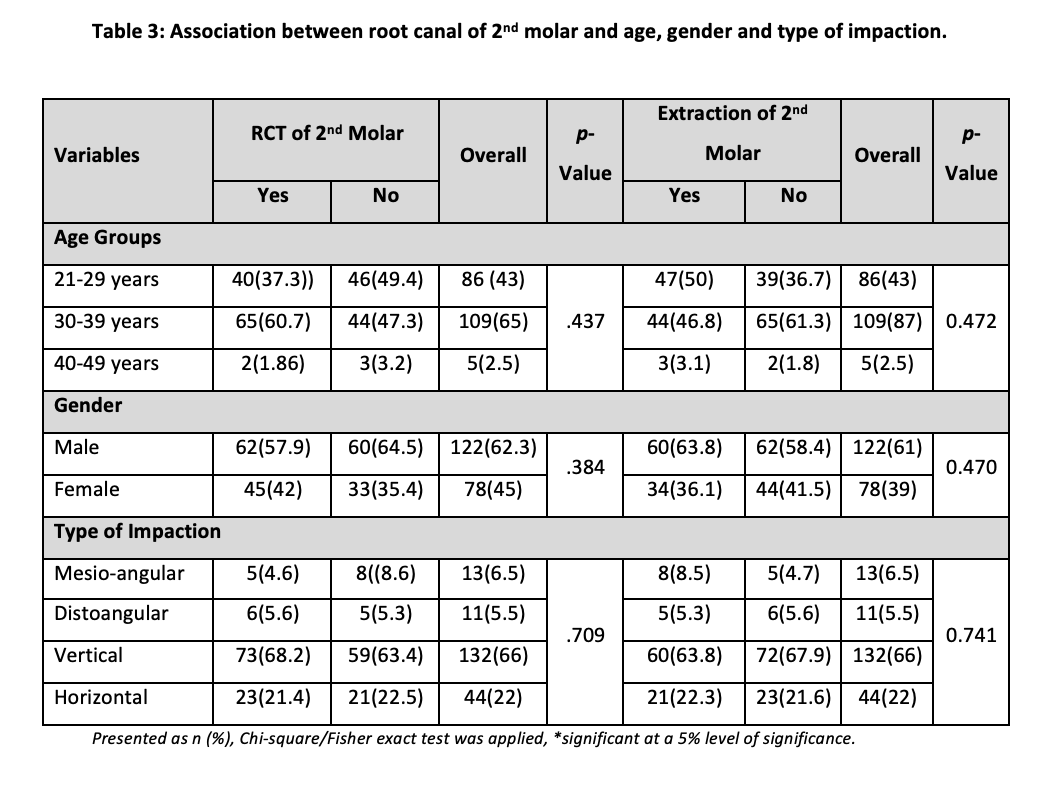
Comparison between distal caries of 2nd permanent molar and angulation of the 3rd permanent impacted molar revealed statistically significant results (p=0.00), while comparison between angulation of 3rd permanent impacted molar with mesial caries in 3rd permanent impacted molar was statistically insignificant (p=0.188). When the relationship between distal caries of 2nd permanent molar and root canal treatment was determined it was observed that the results were statistically insignificant (p=0.563). Moreover, the relationship between distal caries in 2nd permanent molar and extraction was also found to be statistically insignificant (p=0.664).
Some respondents were advised to get their 2nd and 3rd permanent molar extracted while others were advised to get root canal treatment of 2nd permanent molar according to the condition of the tooth (Table 3). A total of 200 patients with impacted 3rd molar underwent extraction. 46.5%, a total of 93 patients underwent root canal treatment for 2nd permanent molar while, 53.5%, the remaining 108 patients got their tooth extracted (Table 3).
In this study, the most common age involved was the third decade. Different parameters such as root canal treatment and extraction of the respective molars were also assessed in this article. There was male predominance in our study. When a tooth’s eruption path is hindered, it is said to be impacted, with the third molar being the most commonly impacted tooth. Obstruction in the route of an eruption of the third molar has been observed due to a variety of reasons, including adjacent teeth, bone, and soft tissue. The pathogenesis of third molar impaction has been linked to a lack of space in the dental arch for the third molar to form, as well as pathological lesions, slowed growth of tooth germs due to nutritional inadequacy, irradiation, and physical trauma1,2,18. Hence, in the current study, we evaluated the frequency of distal caries and assessed the association of distal caries with age, gender and type of impaction. We also assessed the association of type of impaction with age groups and gender.
Mandibular 3rd molars are the last teeth to emerge inside the oral cavity. Primarily, they are common in the age range of 17 to 24 years or as late as the 3rd or 5th decade of life1,2,18. In the present study, the majority of the subjects were in the age range of 30 to 39 years (54.7%), followed by 21 to 29 years (42.8%), respectively and 2.5% were of age 40 to 49 years. This is similar to the study conducted in Saudi Arabia and Iran19,20. While in a similar Pakistani study conducted by Ashar et al. reported that most of the participants were of 23 to 29 years (39.7%), followed by 17 to 22 years (33.08%).15 Another Pakistani study by Rauf et al. also reported the highest frequency of 3rd molar impaction in the 2nd and 3rd decades of life and every few people were of age greater than 40 years16. This might be because of the increasing knowledge about early extraction of impacted 3rd molars and oral health16.
In the current study, males had a high frequency of impacted 3rd molars than females (61.2%, 38.8%). This is similar to the previous study conducted by Syed et al. and Asif and colleagues20, 21. Whereas, evidence shows a significantly greater frequency of impacted 3rd molars in females than in males. These findings are not aligned with the theory of Hellman which stated that the growth of females’ jaws stops when 3rd molars just start to erupt, while males’ jaws continue to grow beyond the eruption time of 3rd molars, leading to a reduction in the incidence of impaction of 3rd molars in males than females16,19,21.
In the current study, the commonest type of impaction was mesio-angular impaction which is similar to previous studies conducted among different ethnicity and populations22,23. Previous Pakistani studies also revealed that mesio-angular impaction was the most common type of impaction15, 24. The prevalence of dental caries in the second molar adjacent to 3rd molars has been estimated to be as less as 1% to 5% to as high as 15% to 51% in previous studies5-7,15. In our study, we also found slightly higher frequency as 61% of distal caries of 2nd molars in the presence of impacted 3rd molars. Ashar et al. found the frequency of distal caries of the 2nd molar was estimated as 40.8% to 42.5% in the presence of impacted mandibular 3rd molars15,24. The variations in the prevalence might be due to regional, racial and/or social-cultural factors13.
In this study, the highest frequency of distal caries was observed among mesio-angular impaction (84.4%). This result is similar to many previous studies showing similar patterns25-27. In an Indian study by Srivastava et al. mesio-angular impaction was significantly associated with distal caries of 2nd molars14. Another study by Sheikh et al. also revealed that the high frequency of caries was related to mesio-angular impaction (41% to 56.3%) 15,24. Hence, mesio-angular impaction of the 3rd molars can cause accumulation of plaque, which resulted in distal caries in the 2nd molars. Thus, the extraction of mesio-angular impaction before the incidence of distal caries could be beneficial for the oral health of the patient.
In the current study, the mesio-angular impaction and disto-angular were more common in males than females. We also observed a significant association between the type of impaction and gender (p=0.048). Other research studies reported a higher frequency of mesio-angular impaction among males, whereas the most frequent impactions reported among females were disto-angular15,24-27. Mesio-angular impactions were frequently found followed by Vertical impactions. Extraction following mesial caries of 3rd permanent molar was found to be prevalent. In this retrospective analysis of OPGs, nutritional and dietary patterns of the patients, co-morbids, and smoking history were not recorded. Overall, oral hygiene status and DMFT score were not calculated in this study. Future studies should be done to see the impact of these etiologies and oral hygiene on the frequency of distal surface of the mandibular 2nd molar in the presence of the impacted 3rd molars. However, further study can be carried out on a large sample size.
The frequency of 2nd molar distal caries was high in the presence of mesio-angular impacted 3rd molars, and it was linked to the type of impaction. As a result, preventative measures like oral hygiene maintenance and 3rd molar extraction in presence of mesio-angular impaction should be implemented to avoid 2nd molar distal caries.
The authors would like to acknowledge the staff of the radiology department for their immense contribution.
The authors declared no conflict of interest.
AA conceived the idea and design of the study; AR did the write-up for the original draft. AB did the data analysis and interpretation, SS revised the manuscript, and NN and AA performed the data collection.
Written consent was taken from the parents of all participants. Anybody who wished to drop in the middle of the study was allowed to do so.
AK and SUS were involved in conceiving the idea, benchwork and writing the manuscript. RA did the statistical analysis. SBA and SUS worked on manuscript writing and proofreading.
- Toedtling V, Coulthard P, Thackray G. Distal caries of the second molar in the presence of a mandibular third molar – a prevention protocol. Br Dent J. 2016;221(6):297-302. doi: 10.1038/sj.bdj.2016.677
- Ventä I, Schou S. Accuracy of the third molar eruption predictor in predicting eruption. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2001;91(6):638-642. doi: 10.1067/moe.2001.113350
- Haddad Z, Khorasani M, Bakhshi M, Tofangchiha M. Radiographic position of impacted mandibular third molars and their association with pathological conditions. Int J Dent. 2021;2021:1-11. doi: 10.1155/2021/8841297
- Chang SW, Shin SY, Kum KY, Hong J. Correlation study between distal caries in the mandibular second molar and the eruption status of the mandibular third molar in the Korean population. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009;108(6):838-843. doi: 10.1016/j.tripleo.2009.07.025
- Tamba B, Tine SD, Ba A, Gassama BC, Niang PA, Diatta M, et al. Difficulty extracting the impacted mandibular third molar: place of the orthopantomogram. Oral Med Oral Surg. 2015;21(3):127-135. doi: 10.1051/mbcb/2015028
- Kaur R, Kumar AC, Garg R, Sharma S, Rastogi T, Gupta VV. Early prediction of mandibular third molar eruption/impaction using linear and angular measurements on digital panoramic radiography: A radiographic study. Indian J Dent. 2016; 7(2): 66-69. doi: 10.4103/0975-962X.184644
- Deshpande P, M VG, Patil K. Proximity of impacted mandibular third molars to the inferior alveolar canal and its radiographic predictors: a panoramic radiographic study. J Maxillofac Oral Surg. 2013;12(2):145-51. doi:10.1007/s12663-012-0409-z
- Ndiaye ML, Gassama BC, Niang SO, Lecor PA, Ndiaye A, Toure B. Distal pathologies of the second molar in the presence of the mandibular third molar: study by panoramic radiography. Adv Oral Maxillofac Surg. 2021;3:1-4. doi: 10.1016/j.adoms.2021.100090
- Syed KB, Alshahrani FS, Alabsi WS, Alqahtani ZA, Hameed MS, Mustafa AB, et al. Prevalence of distal caries in mandibular second molar due to impacted third molar. J Clin Diagn Res. 2017; 11(3): ZC28-ZC30. doi: 10.7860/JCDR/2017/18582.9509
- Özeç İ, Siso ŞH, Taşdemir U, Ezirganli Ş, Göktolga G. Prevalence and factors affecting the formation of second molar distal caries in a Turkish population. Int J Oral Maxillofac Surg. 2009;38(12):1279-1282. doi:10.1016/j.ijom.2009.07.007
- McArdle LW, Renton TF. Distal cervical caries in the mandibular second molar: an indication for the prophylactic removal of the third molar? Br J Oral Maxillofac Surg. 2006;44(1):42-45. doi:10.1016/j.bjoms.2005.07.025
- Al-Khateeb TH, Bataineh AB. Pathology associated with impacted mandibular third molars in a group of Jordanians. J Oral Maxillofac Surg. 2006;64(11):1598-1602. doi:10.1016/j.joms.2005.11.102
- Altiparmak N, Oguz Y, Neto R. Prevalence of distal caries in mandibular second molars adjacent to impacted third molars: a retrospective study using panoramic radiography. J Dent Health Oral Disord Ther. 2017;8(6):641-645. doi: 10.15406/jdhodt.2017.08.00307
- Srivastava N, Shetty A, Goswami RD, Apparaju V, Bagga V, Kale S. Incidence of distal caries in mandibular second molars due to impacted third molars: Nonintervention strategy of asymptomatic third molars causes harm? A retrospective study. Int J Appl Basic Med Res. 2017;7(1):15-19. doi:10.4103/2229-516x.198505
- Ashar T, Shakoor A, Ghazal S, Parveen N, Saleem MN, Raja HZ. Prevalence of distal carious lesions in mandibular second molars due to mesio-angular impacted third molars. J Pak Dent Assoc. 2021;30(1):50-55. doi: 10.25301/JPDA.301.50
- Rauf S, Ali W, Tariq Q, Chaudhry R, Kazmi SS, Imtiaz M. Pattern of mandibular third molar impaction: a radiographic study. Pak Oral Dent J. 2019;39(3):238-242.
- Raheem A, Alhamdani F, Kamal B. The influence of mandibular third molar position on distal caries in mandibular second molar. J Oral Dent Res. 2015;2(1):16-23.
- For the dental patient. Tooth eruption: the permanent teeth. J Am Dent Assoc. 2006;137(1):127. doi: 10.14219/jada.archive.2006.0031
- Hashemipour MA, Tahmasbi-Arashlow M, Fahimi-Hanzaei F. Incidence of impacted mandibular and maxillary third molars: a radiographic study in a Southeast Iran population. Med Oral Patol Oral Cir Bucal. 2013;18(1):e140-145. doi:10.4317/medoral.18028
- Syed KB, Zaheer KB, Ibrahim M, Bagi MA, Assiri MA. Prevalence of impacted molar teeth among Saudi population in Asir Region, Saudi Arabia – A retrospective study of 3 years. J Int Oral Health. 2013;5(1):43-47.
- Asif SA, Syed N, Shah AA, Akhtar MU. Dental caries and pericoronitis associated with impacted mandibulat third molars – A clinical and radiographic study. Pak Oral Dent J. 2014;34(2):268-268.
- Rezaei F, Imani MM, Khavid A, Nabavi A. Patterns of mandibular third molar impaction in an Iranian subpopulation. Braz Res Pediatr Dent Integ Clin. 2020;20:1-9. doi: 10.1590/pboci.2020.099
- Eshghpour M, Nezadi A, Moradi A, Shamsabadi RM, Rezaer NM, Nejat A. Pattern of mandibular third molar impaction: A cross-sectional study in northeast of Iran. Niger J Clin Pract. 2014;17(6):673-677. doi:10.4103/1119-3077.144376
- Sheikh MA, Riaz M, Shafiq S. Incidence of distal caries in mandibular second molars due to impacted third molars-A clinical and radiographic study. Pak Oral Dent J. 2012;32(3):364-364.
- Knutsson K, Brehmer B, Lysell L, Rohlin M. Pathoses associated with mandibular third molars subjected to removal. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1996;82(1):10-17. doi:10.1016/s1079-2104(96)80371-4
- Susarla SM, Blaeser BF, Magalnick D. Third molar surgery and associated complications. Oral Maxillofac Surg Clin North Am. 2003;15(2):177-186. doi:10.1016/s1042-3699(02)00102-4
- Blondeau F, Daniel NG. Extraction of impacted mandibular third molars: postoperative complications and their risk factors. J Can Dent Assoc. 2007;73(4):325-331.
This is an open-access article distributed under the terms of the CreativeCommons Attribution License (CC BY) 4.0 https://creativecommons.org/licenses/by/4.0/