By Saba Raza1, Usman Ali1, Adnan Mustafa Zubairi1, Nida Haider1, Erum Salim2, Aisha Habib1
- Department of Chemical Pathology, Dr. Ziauddin University Hospital, North Nazimabad Campus, Karachi, Pakistan.
- Dr. Ziauddin University Hospital, Clinical Laboratory, Clifton Campus, Karachi, Pakistan.
DOI: https://doi.org/10.36283/PJMD12-2/003
How to cite: Raza S, Ali U, Zubairi AM, Haider N, Salim E, Habib A. Evaluation of Heart Fatty Acid Binding Protein (H-FABP) As A Diagnostic Marker in Acute Coronary Syndrome. Pak J Med Dent. 2022;12(2): 10-15. doi: 10.36283/PJMD12-2/003
Background: Heart Type Fatty Acid Binding Protein (H-FABP) is a biomarker suggested for early detection of Acute Coronary Syndrome (ACS). Early diagnosis and management are critical as it could prevent and reduce morbidity and mortality. The study aimed to determine the diagnostic accuracy of H-FABP as a biomarker of ACS compared to gold standard high-sensitivity Troponin I (hs–TnI) and/or ECG findings suggesting ischemia.
Methods: The study was conducted from May 2020 to November 2020 at Dr. Ziauddin University Hospital in Karachi. Blood samples of 154 patients were collected, who presented to an emergency department or admitted to the Cardiac Care Unit more than 18 years of age with symptoms suggesting angina as pain in the chest, left arm/lower jaw, increased heart rate and shortness of breath. Patient data regarding age, gender, duration of chest pain onset, kidney disease, diabetes mellitus, hypertension and smoking were collected. Serum H-FABP was analyzed on a Quantitative Fluorescence immunoassay Analyzer. Diagnostic accuracy statistics for H-FABP were calculated with the help of contingency tables taking hs-TnI and/or ECG findings as a gold standard.
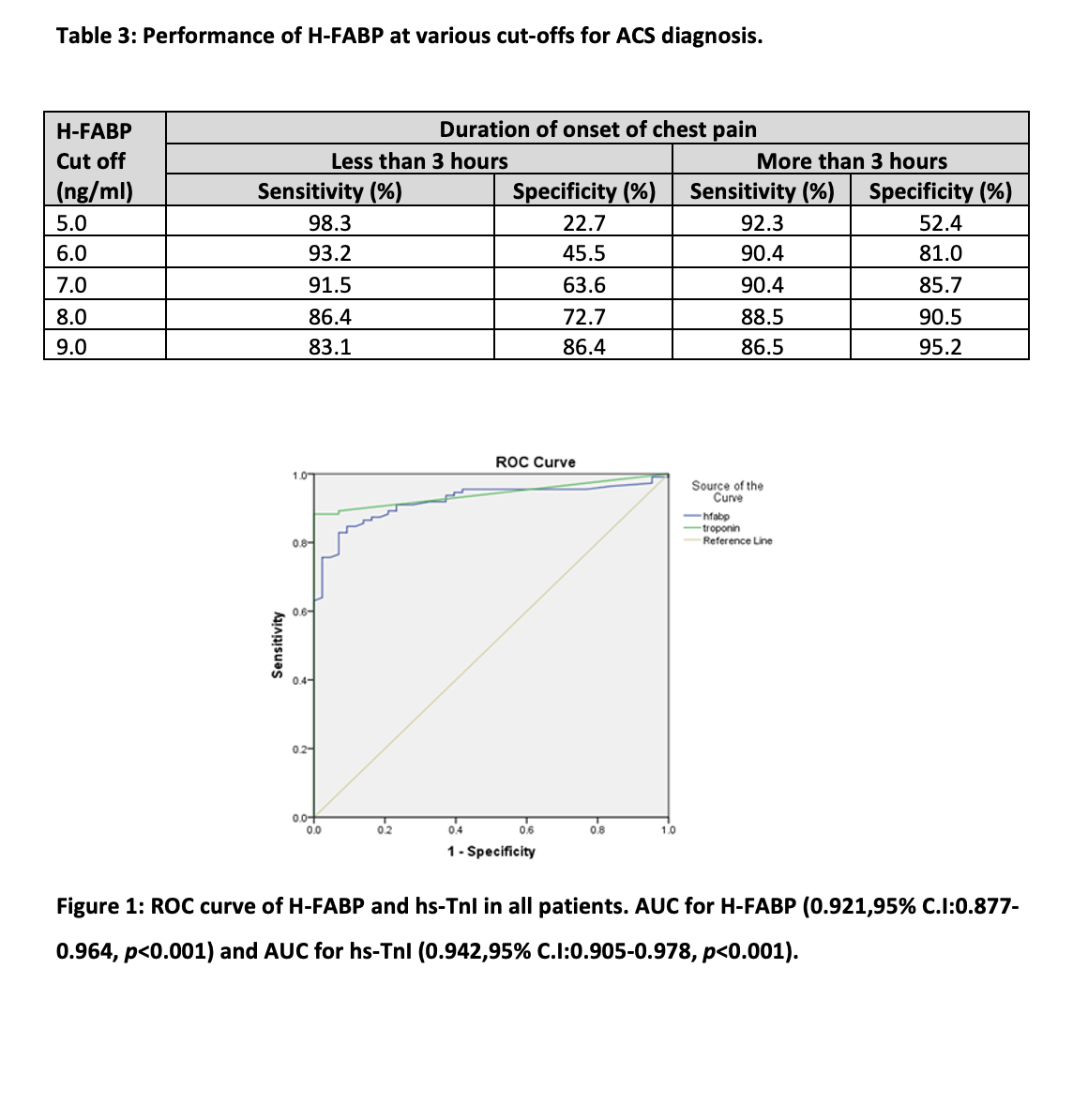
Results: Overall H-FABP showed sensitivity (91.0%), specificity (76.7%), PPV (90.9%), NPV (76.7%) and diagnostic accuracy was 87.58%. H-FABP demonstrated an Area Under Curve (0.911, 95% C.I:0.850-0.972, p<0.001), higher than that of hs-TnI (0.908, 95% C.I:0.844-0.971, p<0.001) in patients having chest pain for 3 hours or less, at the cost of specificity.
Conclusion: H-FABP is a more sensitive biomarker than hs-TnI in the early diagnosis of ACS (p<0.001). However, being less specific, it can be used as an adjuvant cardiac biomarker for early diagnosis of ACS.
Keywords: Diagnostic Accuracy, Acute Coronary Syndrome; Heart-Type Fatty Acid Binding Protein; Cardiac Biomarkers.
Acute Coronary Syndrome (ACS) is a life-threatening occurrence and causes significant morbidity and mortality with a prevalence of 46.8% 1. ACS is considered a spectrum as it includes three clinical presentations i.e., ST-segment elevation myocardial infarction (STEMI), non–ST-segment elevation myocardial infarction (NSTEMI) and unstable angina. According to ESC/ACCF/AHA/WHF Fourth universal definition of myocardial infarction, Cardiac Biomarkers levels, Electrocardiography (ECG) and Coronary Angiography (CAG) findings are required for its diagnosis2. Different markers used in the diagnosis of ACS are Cardiac troponin I (cTnI), Creatine Kinase (CK-MB), Myoglobin and H-FABP 3. Cardiac troponin I (cTnI) is one of the biomarkers recommended for early risk stratification. It is a highly specific marker with a molecular weight of 23.9 KDa, though after the onset of symptoms, cardiac troponin I may not rise for the first 6 hours and require serial measurements within 8–12 hours from onset of pain4,5.
H-FABP is a novel biomarker that is released from the myocardium as a result of its injury. After ischemia onset, its levels are detectable in blood within an hour. H-FABP is involved in the transportation of fatty acids from the cell membrane to mitochondria where oxidation of fatty acids takes place, so it plays a key role in the metabolism of fatty acids6-8. Multiple studies have documented that it is a very sensitive marker in the early detection of myocardial injury and can help in the early initiation of treatment9-12. According to a study, the sensitivity of H-FABP is 89.7% and the specificity of H-FABP is 68% in diagnosing ACS 13.
As the ACS is one of the leading causes of high morbidity and mortality and also has a high economic impact on health care. Early diagnosis and management are not only helpful in reducing mortality but also promise good prognosis and reduce economic burden. Early diagnosis will also reduce the cost incurred due to prolonged hospitalization and the development of complications related to ACS. The purpose of our study was to investigate the diagnostic effectiveness of H-FABP as a biomarker for diagnosis of ACS in different patient groups i.e., gender, chronic diseases, and time from symptom onset in our region (Pakistan). The study aimed to determine the diagnostic accuracy of H-FABP as a biomarker of ACS compared to gold standard high-sensitivity Troponin I (hs–TnI) and/or ECG findings suggesting ischemia.
This was a cross-sectional study conducted from May 2020 to November 2020 in the Department of Chemical Pathology, Dr. Ziauddin University Hospital. One hundred and fifty-four patients from an emergency department or admitted to Cardiac Care Unit with age more than 18 years presented with symptoms suggesting angina such as pain in the chest, left arm or lower jaw, increased heart rate and shortness of breath were included in our study. We excluded those patients from our study who have a history of muscle injury/ trauma for less than three days. Non-probability consecutive sampling was done. The ethical Committee of the Hospital approved our study (2020320SRPAT). The purpose of our study was explained to all patients and after their written consent, a questionnaire was filled out. ACS was diagnosed following ESC/ACCF/AHA/WHF 4th universal definition of myocardial infarction2.
Blood samples for hs-TnI and H-FABP were collected in a lithium heparin tube. Plasma was separated from the primary tubes by centrifuging for 15 minutes at 3000g and plasma was separated into aliquots and stored at -70oC until testing. hs-TnI was analyzed by the Chemiluminescence method on an automated Abbot Alinity Immunoassay analyzer and H-FABP by Finecare Quantitative Fluorescence immunoassay method with appropriate quality controls. Cut-offs of >7 ng/ml were used for H-FABP as indicating risk of Acute Myocardial Infarction and 0.034 ng/ml in males and 0.016 ng/ml in females at 99th percentile was used for hs-TnI as per kit insert.
Statistical analysis was done using SPSS version 22. Median values with percentiles were reported along with mean and standard deviation for quantitative variables such as age, Body Mass Index (BMI), systolic and diastolic blood pressure, H-FABP levels, hs-TnI levels, as the data were not normally distributed. Mann-Whitney test was used to compare the quantitative variables among ACS and non-ACS groups. Effect modifiers such as age, gender, duration of onset of chest pain, Chronic Kidney Disease, Diabetes Mellitus, Hypertension, Cerebrovascular disease, and smoking status were controlled through stratification. Sensitivity, specificity, PPV and NPV and likelihood ratios were derived from the contingency table for the assessment of the diagnostic performance of H-FABP. Receiver Operating Characteristics (ROC) Curve was plotted and AUC was calculated to examine the diagnostic performance of H-FABP and to determine its optimal cut-off. p-value ≤ 0.05 was taken as statistically significant.
The study comprised a total of 154 patients who met the inclusion requirements. The patients had a median age of 59 (50-70) years whereas, 76 (49%) were males and 78 (51%) were females. Out of 154 patients, 91 (59.09 %) had Diabetes Mellitus, 108 (70.12 %) were known to have hypertension, 38 (24.67 %) had a history of smoking, 29 (18.83 %) had a history of cerebrovascular disease, and 29 (18.83 %) had a history of chronic kidney disease. In our study, 111 (72.07%) patients had ACS. Median H-FABP and hs-TnI levels in all patients were 17.8ng/ml (6.6-105.1) and 0.113 ng/ml (0.100-2.068) respectively. Median levels of H-FABP and hs-TnI in the ACS group were found significantly higher than in the non-ACS group with (p-value <0.001) as shown in Table 1.

The overall diagnostic accuracy of H-FABP was 87.58%. Out of 154, 101 patients were true positive (TP), 10 were false positive (FP), 10 were false negative (FN) and 33 were true negative (TN) using a cutoff value of ≥ 7 ng/ml for H-FABP. The sensitivity, Specificity, PPV, NPV and likelihood ratio of H-FABP is shown in Table 2.
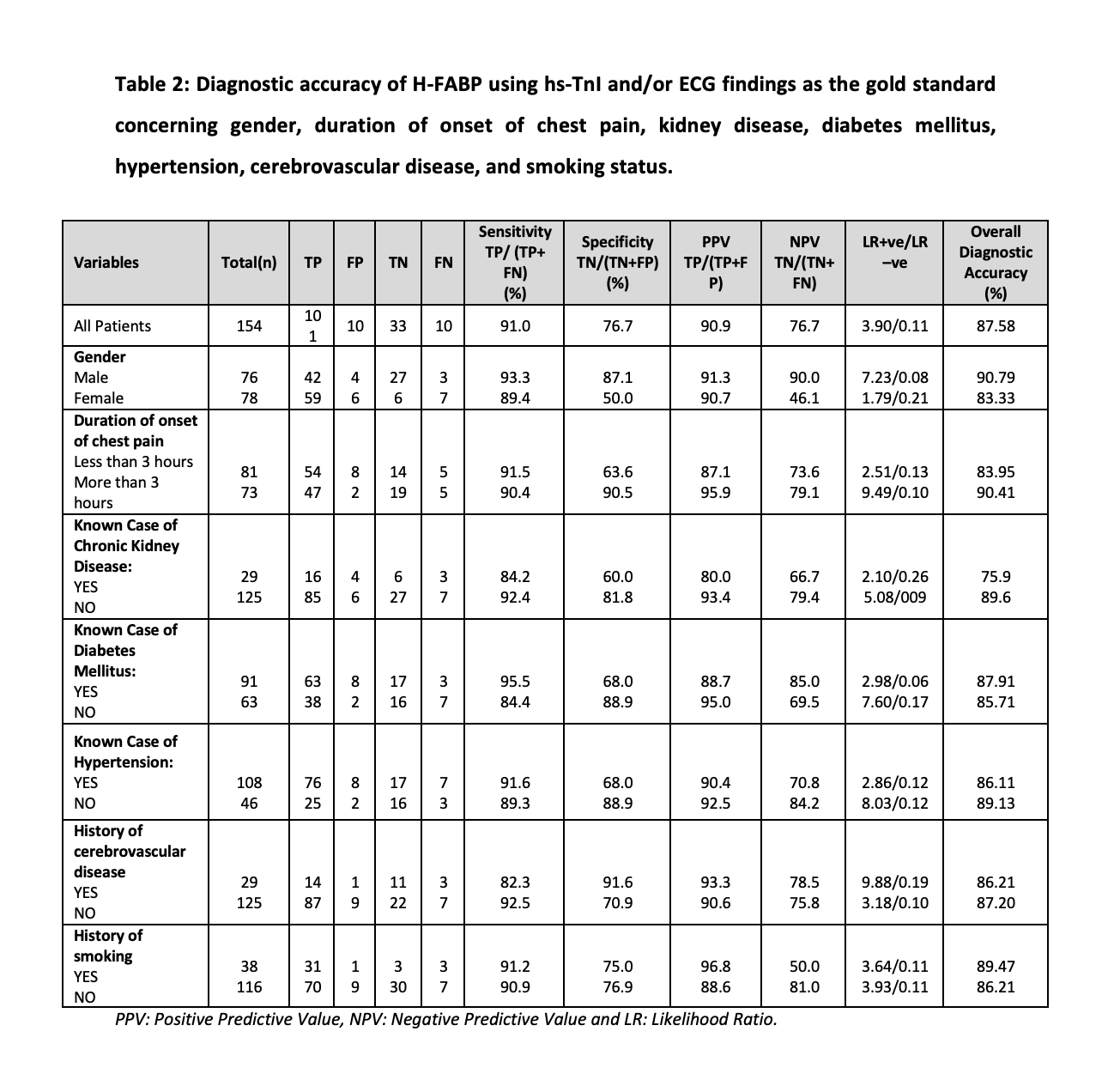
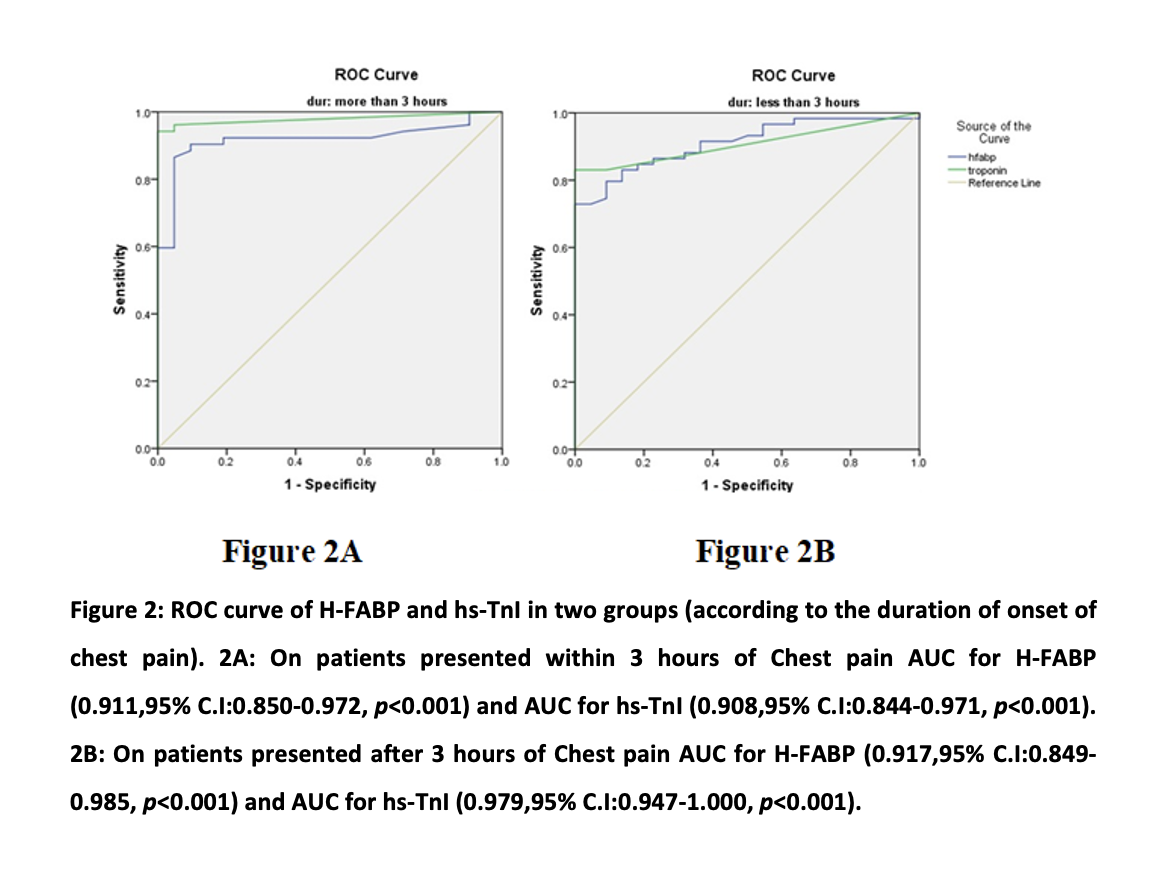
In those patients, who have chest pain for three hours or less, H-FABP showed better diagnostic performance with an AUC of (0.911, 95% C.I:0.850-0.972, p<0.001) higher than that of hs-TnI (0.908,95% C.I:0.844-0.971, p<0.001) (Figure 1 and 2). Diagnostic performance of H-FABP was evaluated at different cut-offs in both groups (i.e., according to the duration of onset of chest pain), maximum sensitivity of 98.3% was observed in those patients, who have chest pain for less than three hours but at cost of specificity which was only 22.7% at a cutoff of 5 ng/ml as shown in Table 3.
In our study, H-FABP had an overall sensitivity of 91.0%, specificity of 76.7%, PPV of 90.9%, and NPV of 76.7%. The LR+ve and LR–ve were found to be 3.90 and 0.11 respectively. One study conducted on 250 patients using a cutoff of 16 ng/ml for H-FABP reported a sensitivity of 85%, specificity of 83.3%, PPV of 96.8%, and much lower NPV of 48.4% when compared to our study. ACS is one of the most common causes of death in the world. Early and accurate diagnosis is extremely important for immediate treatment, thus reducing mortality. Various biomarkers such as Myoglobin, CK-MB, glycogen phosphorylase isoenzyme BB, cardiac Troponin I, etc. play an important role and have been studied for early diagnosis of ACS as an alternative or in conjunction with troponins. Within one to three hours of the onset of symptoms, myoglobin is one of the biomarkers used to diagnose AMI. Myoglobin, on the other hand, is not a specific marker because its concentration in skeletal muscles is much higher than in cardiac tissue. In 1988, H-FABP was first identified as a possible indicator of myocardial injury. Its role as a potential biomarker for immediate myocardial injury and long-term post-ischemic progress has gained interest in recent years14.
The mean age of patients, in our study, was 59 years whereas a study reported mean age of 55 years15. In our study,111(72.07%) patients had ACS as compared to a study that reported a frequency of 136 (68%)16. Our analysis found a statistically significant difference between the ACS and non-ACS groups concerning median levels of H-FABP and hs-TnI. Research conducted by Pyati et al. supplemented this finding17. For cardiac biomarkers, another study found a significant difference between the two groups18.
Mehmood and Khawaja conducted a study in 100 consecutive patients admitted with acute chest pain suggestive of ACS and discovered that H-FABP peak concentration occurred at 8 hours after symptoms onset and was the most sensitive early marker with 79.9%, 98%, and 95.3 % sensitivity at presentation, 2 hours, and 4 hours, respectively. In our study, H-FABP showed overall Diagnostic accuracy of 87.58% which was found to be near similar accuracy (84.4%) reported in other studies15. Another study found sensitivity, specificity, PPV and NPV of H-FABP as 92.6%, 75%, 88.7% and 82.7% respectively16. A study conducted in 2018 used a cutoff of 7.15 ng/ml for H-FABP, comparable to our study, as we used a cutoff of 7ng/ml and reported 51.5% sensitivity, 96.3% specificity and 68.3 % diagnostic accuracy, which was low compared to our study19. This may be due to the effect of different variables and the diversity in the demographics and settings of the sample.
This study’s results showed that for patients who have chest pain for three hours or less, H-FABP has a sensitivity of 91.5% which was higher than the sensitivity of troponin I of 83.0%, this highlights an important aspect as high sensitivity is important for the early ‘rule in’ of disease. However, the specificity of H-FABP was lower (63.6%) than that of hs-TnI (91%). In a group of patients, who presented with chest pain three hours after its onset, the specificity of H-FABP raised to 90.5% which was comparable to the specificity of hs-TnI (91%). The findings of a study done by Kabekkodu et al. were consistent with our study20. while contrary to it, a study conducted by Elmadbouh et al. revealed no difference in sensitivity of H-FABP and cTnI and lower specificity of cTnI in patients having chest pain for three hours or less. This difference may be attributed to the lack of standardization of the H-FABP assay and different cutoff values used for diagnosis21.
By using AUC and ROC as a measure of test performance of H-FABP and hs-TnI in two groups (according to the duration of the start of chest pain), H-FABP achieved a higher AUC (0.911, 95% C.I:0.850-0.972, p<0.001) in patients having chest pain for three hours or less, followed by hs-TnI (AUC 0.908, 95% C.I:0.844-0.971, p<0.001). This finding in our analysis is supplemented by a study of Kabekkodu et al. in which H-FABP showed better performance than cTnI within the first four hours of myocardial injury20. A study found that AUC for H-FABP and high-sensitive Troponin T (hs-TnT) was 0.885(0.79-0.94) and 0.805(0.70-0.88) in the initial six hours of symptoms respectively22. Orak et al. in a study conducted on 100 consecutive patients admitted with acute chest pain suggestive of ACS discovered that H-FABP was the most sensitive early marker with 79.9%, 98%, and 95.3% sensitivity at presentation, two hours, and four hours, respectively23. Better performance in the early onset of chest pain may be due to an early release of H-FABP into the systemic circulation from damaged myocardium because it is small in size and freely located in cytoplasm24-26. Our study has a few drawbacks, such as a lack of multicenter data collection and we have not been able to conduct serial measurements of cardiac markers to evaluate their kinetics.
The study found that H-FABP demonstrated greater sensitivity in chest pain within 3 hours. It can be utilized along with hs-TnI to diagnose ACS in an early phase of ischemia. However, its specificity was lower than that of High sensitivity cardiac troponin I (hs-cTnI), so it could not be used as a sole biomarker to diagnose ACS.
The authors would like to acknowledge Mr. Akbar Ali for his assistance in the sample analysis.
There is no conflict of interest to be declared.
The study approval was obtained from the Ethics Review Committee of the Ziauddin University Hospital.
Verbal and written informed consent was obtained from all patients.
All authors contributed equally to this research write-up.
- Lashari NA, Lakho NI, Memon SA, Ahmed A, Waseem MF. Acute coronary syndrome; frequency, contributing factors and types in patient with typical chest pain. Professional Med J. 2017;24(03):409-413. doi: 10.17957/TPMJ/17.3409
- Thygesen K, Alpert JS, Jaffe AS, Chaitman BR, Bax JJ, Morrow DA, et al., Executive Group on behalf of the Joint European Society of Cardiology (ESC)/American College of Cardiology (ACC)/American Heart Association (AHA)/World Heart Federation (WHF) Task Force for the Universal Definition of Myocardial Infarction. Fourth universal definition of myocardial infarction (2018). Circulation. 2018;138(20): e618-e651. doi: 10.1161/CIR.0000000000000617
- Jacob R, Khan M. Cardiac biomarkers: what is and what can be. Indian J Cardiovasc Dis Women WINCARS. 2018;3(04):240-244. doi: 10.1055/s-0039-1679104
- Abbasi WA, Saleem M, Rashid S, Kayani AM. Utility of heart type fatty acid binding protein (H-FABP) point of care test in the early hours of STEMI compared with troponin-I in Pakistani population. J Ayub Med Coll Abbottabad. 2017;29(1):107-111.
- Ye XD, He Y, Wang S, Wong GT, Irwin MG, Xia Z. Heart-type fatty acid binding protein (H-FABP) as a biomarker for acute myocardial injury and long-term post-ischemic prognosis. Acta Pharmacol Sin. 2018; 39(7): 1155-1163. doi: 10.1038/aps.2018.37
- Suresh K, Abarna Devi S, Badrinath AK, Suresh Babu S, Nagalingam S. Diagnostic utility of heart type fatty acid binding protein (H-FABP) versus cardiac troponin I in myocardial infarction. Int J Adv Med. 2018; 5:514-519. doi: 10.18203/2349-3933.ijam20181481
- Rezar R, Jirak P, Gschwandtner M, Derler R, Felder TK, Haslinger M, et al. Heart-type fatty acid-binding protein (H-FABP) and its role as a biomarker in heart failure: what do we know so far? J Clin Med. 2020;9(1):1-14. doi: 10.3390/jcm9010164
- Mueller C. Biomarkers and acute coronary syndromes: an update. Eur Heart J. 2013;35(9):552-556. doi: 10.1093/eurheartj/eht530
- Banu S, Tanveer S, Manjunath CN. Comparative study of high sensitivity troponin T and heart-type fatty acid-binding protein in STEMI patients. Saudi J Biol Sci. 2015;22(1):56-61. doi: 10.1016/j.sjbs.2014.05.011
- Liu Y, Jiang Z, Luo J, Peng X, Yi Z. Clinical study of H-FABP for risk stratification and prognosis in patients with early cTnT-negative ACS. Int J Clin Exp Med. 2017;10(3):4873-4880.
- Reda AA, Moharram MA, Soliman MA. Role of heart fatty acid-binding protein (h-FABP-type III) as a diagnostic biomarker in acute coronary syndrome. Menoufia Med J. 2016;29:73-78. doi: 10.4103/1110-2098.178990
- Ramaiah JH, Ramegowda RT, Ashalatha B, Ananthakrishna R, Nanjappa MC. Heart-type fatty acid-binding protein (h-fabp) as a novel biomarker for the early diagnosis of acute myocardial infarction in comparison with cardiac troponin T. J Evol Med Dent Sci. 2013;2(1):16-27.
- Vupputuri A, Sekhar S, Krishnan S, Venugopal K, Natarajan K. Heart-type fatty acid-binding protein (H-FABP) as an early diagnostic biomarker in patients with acute chest pain. Indian Heart 2015;67(6):538-542. doi: 10.1016/j.ihj.2015.06.035
- Ye XD, He Y, Wang S, Wong GT, Irwin MG, Xia Z. Heart-type fatty acid binding protein (H-FABP) as a biomarker for acute myocardial injury and long-term post-ischemic prognosis. Acta Pharmacol Sin. 2018; 39(7): 1155-1163. doi: 10.1038/aps.2018.37
- Mehmood ZM, Khawaja TF. The role of human heart-type Fatty Acid Binding Protein in the early detection of myocardial injury in Acute Coronary Syndrome. J Rawalpindi Med Coll. 2020;24(1):12-16.
- Hamza M, Demerdash S, Ibrahim M. Heart-type fatty acid-binding protein as a diagnostic biochemical marker for early detection of myocardial infarction. Acta Cardiologica. 2016;71(5):537-541. doi: 10.1080/AC.71.5.3167496
- Pyati AK, Devaranavadagi BB, Sajjannar SL, Nikam SV, Shannawaz M. Heart-type fatty acid binding protein: a better cardiac biomarker than CK-MB and myoglobin in the early diagnosis of acute myocardial infarction. J Clin Diagn Res. 2015; 9(10): BC08-BC11. doi: 10.7860/JCDR/2015/15132.6684
- Banu KY, Erdem C, Afşin DH, Özlem U, Yasemin Ç, Afsin I. Value of heart-type fatty acid-binding protein (H-FABP) for emergency department patients with suspected acute coronary syndrome. Afr Health Sci. 2014;14(3):757-762. doi:10.4314/ahs.v14i3.36
- Sotoudeh Anvari M, Karimi M, Shafiee A, Boroumand M, Bozorgi A, Sedaghat R, et al. Complementary diagnostic value of heart type fatty acid-binding protein in early detection of acute myocardial infarction. Crit Pathw Cardiol. 2018;17(1):43-46. doi: 10.1097/HPC.0000000000000107
- Kabekkodu SP, Mananje SR, Saya RP. A study on the role of heart type fatty acid binding protein in the diagnosis of acute myocardial infarction. J Clin Diagn Res. 2016; 10(1): OC07-OC10. doi: 10.7860/JCDR/2016/15713.7057
- Elmadbouh I, Mahfouz R, Bayomy N, Faried W, Ghanayem N. The value of human heart-type fatty acid-binding protein in the diagnosis of patients with acute chest pain. Egypt Heart J. 2012;64(4):179-184. doi: 10.1016/j.ehj.2012.06.004
- Gami BN, Patel DS, Haridas N, Chauhan KP, Shah H, Trivedi A. Utility of heart-type fatty acid binding protein as a new biochemical marker for the early diagnosis of acute coronary syndrome. J Clin Diagn Res. 2015; 9(1): BC22-BC24. doi: 10.7860/JCDR/2015/11006.5451
- Orak M, Üstündağ M, Güloğlu C, Özhasenekler A, Alyan Ö, Kale E. The role of the heart-type fatty acid binding protein in the early diagnosis of acute coronary syndrome and its comparison with troponin I and creatine kinase-MB isoform. Am J Emerg Med. 2010;28(8):891-896. doi: 10.1016/j.ajem.2009.05.012
- Lichtenauer M, Jirak P, Wernly B, Paar V, Rohm I, Jung C, et al. A comparative analysis of novel cardiovascular biomarkers in patients with chronic heart failure. Eur J Intern Med. 2017;44:31-38. doi: 10.1016/j.ejim.2017.05.027
- Das UN. Heart-type fatty acid-binding protein (H-FABP) and coronary heart disease. Indian Heart J. 2016; 68(1):16-18. doi: 10.1016/j.ihj.2015.07.030
- Nguyen TN, Le PX, Le TX, Nguyen KD, Nguyen TT, Nguyen TM, Tran VT. The value of heart-fatty acid binding protein (H-FABP) in the early diagnostic of patients with acute myocardial infarction. J Am Coll Cardiol. 2020;75(11_Supplement_1):18-18.
This is an open-access article distributed under the terms of the CreativeCommons Attribution License (CC BY) 4.0 https://creativecommons.org/licenses/by/4.0/