By Mazhar Shafiq1, Shumaila2, Tariq Jaffar3, Sadaf Saleem Uppal4, Akhter5, Farrukh Nadeem6, Muhammad Ali Mazhar7
AFFLIATIONS:
- Department of Radiology, CMH Kohat Cantt, Pakistan.
- Department of Radiology, Shalamar Hospital, Lahore, Pakistan.
- PNS Hospital Shifa, Karachi, Pakistan.
- Department of Biochemistry, Shalamar Medical and Dental College, Lahore, Pakistan.
- Department of Radiology, CMH, Bahawalpur, Pakistan.
- Department of Radiology, CMH, Lahore, Pakistan.
- Central Park Medical College, Lahore, Pakistan.
DOI: https://doi.org/10.36283/PJMD11-4/005
ORCID iD: 0000-0001-8325-365X
How to cite: Shafiq M, S, Jaffar T, Uppal SS, Nadeem F, Mazhar MA, et al. Incidental Detection of Thyroid Nodule on Carotid Color Doppler Ultrasound in Patients Presenting with Cerebrovascular Diseases. Pak J Med Dent. 2022;11(4): 29-33. doi: 10.36283/PJMD11-4/005
Background: Thyroid nodules are often detected in clinical practice, during physical examination, or accidentally during different imaging techniques. Most of these nodules are characterized as benign, and thyroid cancer is identified in only a small subclass. Ultrasonography is considered an important tool in thyroid nodule evaluation. Therefore, the study aimed to determine the frequency of incidental detection of a nodule of thyroid on carotid color Doppler ultrasound in patients presenting with cerebrovascular diseases.
Methods: A cross-sectional descriptive study was carried out in the PNS Shifa hospital, Radiology department, from August 2017 to May 2018. Patients (n=110) underwent Color Doppler Ultrasound examinations with a scanner (Xario), furnished with a linear transducer operational at 10 MHz by the researcher. Incidental detection of thyroid nodule was labeled. Demographic detail including name, age, gender, and BMI was noted. Echogenicity and size of the thyroid gland was compared to that of encompassing glandular parenchyma. The data collected were analyzed and interpreted using SPSS version 20.
Results: The patient’s mean age was 59.92 ± 11.03 years with the ratio being 1.2:1 between males and females respectively. Diabetes and hypertension were existent in 43(39.1%) and 54(49.1%) patients respectively. Family history of thyroid nodules was present in 31(28.2%) patients. Thyroid nodule was detected in 34(30.91%) patients. The Benign pattern of thyroid nodules on grayscale. However, the histologic pattern of a mildly differentiated follicular thyroid carcinoma was detected.
Conclusion: The frequency of incidental detection of thyroid nodule on carotid color Doppler ultrasound was 30.91% in patients presenting with cerebrovascular diseases.
Keywords: Carotid Color Doppler Ultrasound; Incidental Detection; Cerebrovascular; Thyroid Nodule.
Iodine is fundamental for the synthesis of thyroid hormones. Its deficiency leading to goiter occurs in 2.7% of the global population as of the 2010 report1. In Pakistan, the prevalence of iodine deficiency is 63.6% following the WHO database2. A thyroid nodule is a distinct lesion specific to the thyroid gland3. The occurrence of thyroid nodules is 4% to 7% on palpation alone and 18% to 67% on ultrasonography assessment. However, fewer than 7% of these nodules are malignant neoplasms4,5.
Ultrasound imaging has developed as an imperative analytical tool in the evaluation of thyroid nodules. It is extremely sensitive for nodule detection, and the ultrasound attributes of the nodules can be employed to decide the requisite for additional exploration. Quite a few studies have studied the benign and malignant ultrasound imaging characteristics of thyroid nodules5. High-resolution ultrasonography with Doppler is a useful and reliable tool to segregate benign from malignant thyroid nodules6. Research has shown that the possibility of malignancy is higher in nodules with a completely central vascular pattern while nodules with a primarily perinodular pattern are more benign 7.
The thyroid nodules are identified parenthetically during the physical evaluation and imaging of the neck for different purposes8. Thyroid incidentaloma is a term used to define coincidental thyroid nodules detection by medical imaging studies planned for other reasons. The stated prevalence of incidental thyroid nodule detection during Doppler ultrasound studies vary significantly depending upon the age of the patient, use of added iodine, and other less imperative factors9,10. The prevalence of thyroid incidentaloma by other imaging techniques and its clinical importance has been stated by numerous prior studies. The increased use of different imaging modalities, such as ultrasound, computed tomography and magnetic resonance imaging have shown a steady increase in the prevalence of thyroid incidentaloma. In a contrast-enhanced MR angiography study, incidental thyroid nodules were detected in 4.6% of patients11,12.
Cerebrovascular diseases are medical conditions that affect cerebral circulation. The most common presentation is an ischemic stroke and occasionally a hemorrhagic stroke. The color Doppler ultrasound is a widely recognized evaluation tool for the carotid artery and its branches. The thyroid gland is positioned in the neck in close vicinity to the carotid vessels13. Assessment of the thyroid gland during the carotid Doppler ultrasound imaging is a cost-effective, non-tedious method that may have diagnostic advantages14.
The rationale of the study is to determine the frequency of incidental detection of thyroid nodules on carotid color Doppler ultrasound in patients presenting with cerebrovascular diseases. This help in attaining the local magnitude of this problem as well as in updating local guidelines for early detection and prevention of thyroid disease in the local population. The study aimed to determine the frequency of incidental detection of thyroid nodule on carotid color Doppler ultrasound in patients presenting with cerebrovascular diseases.
A cross-sectional study was carried out after synopsis approval at the radiology department of PNS Shifa hospital. The sample size of 110 patients was calculated with a confidence level of 95%, 9.5% error margin, and taking an anticipated percentage of incidental thyroid nodule i.e., 51.1% in patients undergoing Color Doppler Ultrasound. The study approval was obtained by the institutional ethics review board and informed consent was taken from patients.
The sampling method was non-probability sampling at convenience. Inclusion criteria were patients between 40-80 years of age belonging to either gender with a diagnosis of cerebrovascular disease referred for Color Doppler Ultrasound. Patients with previously known thyroid disease, malignancy, or surgery (on medical record) were added to the exclusion criteria. A total of 110 patients referred to the Radiology Department of the hospital and satisfying the selection criterion were registered for the study. Demographic detail (name, age, gender, and BMI) was noted. The information was recorded and analyzed by version 20.0 of SPSS.
The patients underwent Color Doppler ultrasound examinations with an available scanner (Xario), fortified with a straight transducer operational at 10 MHz by the researchers. Echogenicity and size of the thyroid gland and any focal anomaly (echogenicity of nodule relative to neighboring strap muscles), existence or non-existence of echogenic foci, border depiction (irregular or lobulated), size and type of thyroid nodule i.e., solid (hyperechoic or hypoechoic), cystic (anechoic) or mixed (heterogeneous) as indicated by internal sonographic appearance comparative to that of encompassing glandular parenchyma was recorded. Incidental detection of thyroid nodule was labeled. All this information was recorded on a proforma.
According to the study results, the patient’s mean age was 59.92 ± 11.03 years with the ratio being 1.2:1 between males and females respectively. Of the patients with DM were 43(39.1%) and hypertension was found in 54(49.1%) patients. The study exhibited that the patients with smoking status were 31(29.2%) and the patients without smoking habits were 79(71.8%) as shown in Table 1.
Table 1: Frequency of diabetes mellitus, hypertension, smoking and family history.
| Variables | Female | Male | p-Value |
| Diabetes mellitus
n=43 |
25 | 18 | 0.03 |
| Hypertension
n=54 |
22 | 32 | 0.07 |
| Smoking
n=31 |
0 | 31 | 0.02 |
| Family History
n=31 |
15 | 16 | 1.02 |
In this study, the history of thyroid nodules in the family was present in 31(28.2%) patients and 79(71.8%) of the patients had no history of thyroid nodules in the family. Thyroid nodule was present in 34(30.91%) patients. The single nodule was existent in 18(16.4%) patients and multiple nodules were existent in 16(14.5%) patients. The solid type of nodule was noted in 13(11.8%) patients, cystic type in 10(9.1%) patients and mixed type in 11(10%) patients as shown in Table 2. The mean nodule size of the patients was 1.41±0.48 cm with minimum and maximum values of 0.5 and 2.0 cm respectively.
Table 2: Frequency distribution of number and type of nodules (n=34).
| Number of Nodules | Single | Multiple | |
| 18(16.4%) | 16(14.5%) | ||
| Type of nodule | Solid | Cystic | Mixed |
| 13(38.2%) | 10(29.4%) | 11(32.4%) | |
The study results showed a statistically significant difference between gender and thyroid nodule status i.e., p-value=0.001 and a non-significant difference was found between the age and BMI with thyroid nodule status i.e., p-value >0.05 as shown in Table 3. Within the context of ultrasound, the Benign pattern of thyroid nodules on grayscale is shown in Figure 1. However, the histologic pattern of a mildly differentiated follicular thyroid carcinoma (FTC) (250 X) is presented in Figure 2.
Table 3: Comparison of age, gender and Body mass index (BMI) with a thyroid nodule.
| Comparative Variables | Thyroid Nodule | Total | p-Value | ||
| Yes | No | ||||
| Age (years) | ≤ 60 | 18 | 40 | 58 | 0.976 |
| > 60 | 16 | 36 | 52 | ||
| Gender | Male | 34 | 26 | 60 | 0.001 |
| Female | 0 | 50 | 50 | ||
| BMI | Normal | 13 | 19 | 32 | 0.158 |
| Abnormal | 21 | 57 | 78 | ||

Figure 1: Benign pattern of thyroid nodules on grayscale ultrasound.
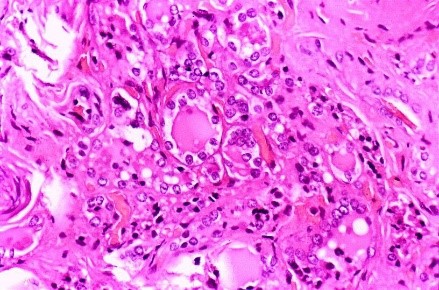
Figure 2: Histologic pattern of a mildly differentiated follicular thyroid carcinoma (FTC) (250 X).
This present cross-sectional descriptive study was done at PNS Shifa hospital, Karachi in the Department of Radiology, to determine the frequency of coincidental detection of thyroid nodule on color Doppler ultrasound of carotid in patients presenting with cerebrovascular. The thyroid nodule is a common entity. An endocrinologist frequently evaluates these nodules because they may epitomize malignancy. The nodules are usually detected on physical examination or incidentally when imaging techniques are executed for other purposes. Ultrasonography is considered the optimal investigation for thyroid nodules. It is a non-invasive technique that can detect small non-palpable nodules, their consistency, the presence of multiple nodules, lateral or central lymphadenopathy of the neck, and offers precise dimensions of nodule diameter for monitoring15. It also has a prime role in the effective treatment of thyroid nodules.
In our study, the frequency of thyroid nodules was 34(30.91%). The frequency of thyroid nodules was significantly greater in female patients as compared to male patients (p=0.001). Different studies have reported the coincidental detection of thyroid nodules during Doppler ultrasound and their prevalence varies significantly depending upon the age of the patient, use of iodine supplementation, and other less imperative factors9, 10.
An ultrasound examination study involving 300 patients without clinical presentation of thyroid disease, showed small, echoic nodules in 17% of male and 20% of female patients with an average of 19% 16. In another study conducted in Iran at least, a single thyroid nodule was identified in 161 (51%) subjects, who were referred for Doppler ultrasound imaging for cervical vessel evaluation17. Bartolotta et al. in their screening of 704 elderly patients with high-resolution ultrasound and real-time spatial compound imaging reported 58.5% and 41.5% thyroid nodules in women and men respectively with the highest prevalence in the 7th decade18.
Rad et al. in their study on 209 patients presented that 63 (21.8%) had abnormal thyroid and incidental thyroid nodules were present in 57 (19.6%) patients; mostly female and elderly. A total of 15 patients underwent fine needle aspiration biopsy (FNAB) and three had significant findings suggestive of neoplasm19. The present study showed a statistically significant difference between gender and thyroid nodule status with p=0.001. Thirty-four out of 60 males (56.66%) had thyroid nodule while thyroid nodule was not detected in any female. However, in our study, no significant difference was detected between age and thyroid nodule status.
In the present study single and multiple nodules were detected in 16.4% and 14.5% of patients respectively. A total of 9.1% of patients had the cystic type of lesion while solid and mixed lesions were detected in 11.8% and 10% of patients respectively. In a study conducted by Steele et al. patients undergoing carotid Doppler Ultrasound, thyroid abnormalities were identified in 9.4% of patients. Nodules were both unilateral and bilateral20. However, the consistency of the lesions was different from our study and was as follows: cystic (47%), solid (43%), and mixed (10%). After biopsy 9 patients were found to have thyroid neoplasm.
In a local study, the frequency of incidental detection of thyroid nodules was 21% in patients who underwent ultrasound examination of their thyroid and were asymptomatic for thyroid disease. Thyroid nodule was present in 16% of males and 25% of females. Among them, 55% had a single thyroid nodule while multiple nodules were present in 45% of patients21. Another study of Carotid Doppler ultrasound on asymptomatic patients documented thyroid nodules in 9.4% of patients. It reported 5(62.07%) and 3 (37.93%) female and male patients respectively22. However, in the current study thyroid nodule was detected in male patients and 53% had single and 47% had multiple nodules.
The frequency of incidental thyroid nodule detection was 30.91% on carotid color doppler ultrasound in patients presenting with cerebrovascular disease. The study observed the frequency of thyroid nodules to be high in patients with cerebrovascular disease. There may be higher chances of thyroid problems in ill patients if more sample size was obtained. We recommend the patients for screening for thyroid nodules because this will assist in improving the current practices and will also update the local guidelines for early detection and prevention of thyroid disease in the Pakistani population.
The authors would like to acknowledge the hospital staff for their assistance and facilitation in the data collection process.
The authors declared no conflict of interest.
The study approval was obtained by the institutional ethics review board.
Informed consent was taken from the patients.
MS contributed to the analysis and interpretation of data, drafted the manuscript, and finalized the paper to be published. TJ and S assisted in the concept and study design, analysis and interpretation of data and drafting of the manuscript. SSU, A, FN and MAM helped in the critical revision and drafting of the manuscript. All authors agreed to be accountable for all aspects of the work.
- Vos T, Flaxman AD, Naghavi M, Lozano R, Michaud C, Ezzati M, et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2163-2196. doi: 10.1016/S0140-6736(12)61729-2
- Mohammadi M, Azizi F, Hedayati M. Iodine deficiency status in the WHO Eastern Mediterranean Region: A systematic review. Environ Geochem Health. 2018;40(1):87-97. doi: 10.1007/s10653-017-9911-z
- Xie C, Cox P, Taylor N, LaPorte S. Ultrasonography of thyroid nodules: a pictorial review. Insights Imaging. 2016 ;7(1):77-86. doi: 10.1007/s13244-015-0446-5
- Yunus M, Ahmed Z. Significance of ultrasound features in predicting malignant solid thyroid nodules: need for fine-needle aspiration. J Pak Med Assoc. 2010;60(10):848-853.
- Hambly NM, Gonen M, Gerst SR, Li D, Jia X, Mironov S, et al. Implementation of evidence-based guidelines for thyroid nodule biopsy: a model for establishment of practice standards. Am J Roentgenol. 2011 ;196(3):655-660. doi: 10.2214/AJR.10.4577
- Chung J, Lee YJ, Choi YJ, Ha EJ, Suh CH, Choi M, et al. Clinical applications of Doppler ultrasonography for thyroid disease: consensus statement by the Korean Society of Thyroid Radiology. Ultrasonography. 2020; 39(4): 315-330. doi: 10.14366/usg.20072
- Mendelson AA, Tamilia M, Rivera J, Hier MP, Sherman M, Garfield N, et al. Predictors of malignancy in preoperative nondiagnostic biopsies of the thyroid. J Otolaryngol. 2009;38(3): 395-400.
- Popoveniuc G, Jonklaas J. Thyroid nodules. Med Clin North Am. 2012; 96(2): 329-349. doi: 10.1016/j.mcna.2012.02.002
- Gharib H, Papini E, Paschke R, Duick DS, Valcavi R, Hegedüs L, et al. American Association of Clinical Endocrinologists, Associazione Medici Endocrinologi, and European Thyroid Association medical guidelines for clinical practice for the diagnosis and management of thyroid nodules: executive summary of recommendations. J Endocrinol Invest. 2010 ;33(5):287-291. doi: 10.1007/BF03346587
- Gharib H, Papini E, Paschke R. Thyroid nodules: a review of current guidelines, practices, and prospects. Eur J Endocrinol. 2008;159(5):493-505. doi: 10.1530/EJE-08-0135
- Lim HK, Park ST, Ha H, Choi SY. Thyroid nodules detected by contrast-enhanced magnetic resonance angiography: prevalence and clinical significance. PLoS One. 2016;11(2):1-10. doi: 10.1371/journal.pone.0149811
- Drake T, Gravely A, Westanmo A, Billington C. Prevalence of thyroid incidentalomas from 1995 to 2016: a single-center, retrospective cohort study. J Endocr Soc. 2020;4(1):1-8. doi: 10.1210/jendso/bvz027
- Gaitini D, Soudack M. Diagnosing carotid stenosis by Doppler sonography: state of the art. J Ultrasound Med. 2005;24(8):1127-1136. doi: 10.7863/jum.2005.24.8.1127
- Sheth S. Role of ultrasonography in thyroid disease. Otolaryngol Clin North Am. 2010;43(2):239-255. doi: 10.1016/j.otc.2010.02.001
- Bomeli SR, LeBeau SO, Ferris RL. Evaluation of a thyroid nodule. Otolaryngol Clin North Am. 2010;43(2):229-238. doi: 10.1016/j.otc.2010.01.002
- Woestyn J, Afschrift M, Schelstraete K, Vermeulen A. Demonstration of nodules in the normal thyroid by echography. Br J Radiol. 1985;58(696):1179-1182. doi: /10.1259/0007-1285-58-696-1179
- Acar T, Ozbek SS, Acar S. Incidentally discovered thyroid nodules: frequency in an adult population during Doppler ultrasonographic evaluation of cervical vessels. Endocrine. 2014;45(1):73-78. doi: 10.1007/s12020-013-9949-3
- Bartolotta TV, Midiri M, Runza G, Galia M, Taibbi A, Damiani L, et al. Incidentally discovered thyroid nodules: incidence, and greyscale and colour Doppler pattern in an adult population screened by real-time compound spatial sonography. Radiol Med. 2006 ;111(7):989-998. doi: 10.1007/s11547-006-0097-1
- Rad MP, Zakavi SR, Layegh P, Khooei A, Bahadori A. Incidental thyroid abnormalities on carotid color doppler ultrasound: frequency and clinical significance. J Med Ultrasound. 2015;23(1):25-28. doi: 10.1016/j.jmu.2014.04.005
- Steele SR, Martin MJ, Mullenix PS, Azarow KS, Andersen CA. The significance of incidental thyroid abnormalities identified during carotid duplex ultrasonography. Arch Surg. 2005;140(10):981-985. doi:10.1001/archsurg.140.10.981
- Kamran M, Hassan N, Ali M, Ahmad F, Shahzad S, Zehra N. Frequency of thyroid incidentalomas in Karachi population. Pak J Med Sci. 2014;30(4):793-797. doi: 10.12669/pjms.304.4808
- Rayyan A. Kinsara, Eman S. Badawod, Maria A. Bagais, Huda A. Saimaldahar, Mohammed A. Alariefy, Adel K. Kotb, et al. Incidental finding of thyroid nodules detected during carotid color doppler ultrasound in asymptomatic patients. Int J Healthcare Sci. 2016;4(2):1914-1916.
This is an open-access article distributed under the terms of the CreativeCommons Attribution License (CC BY) 4.0 https://creativecommons.org/licenses/by/4.0/