By Usman Qureshi, Ramla Ghazanfer, Syed Waqas Hasan, Hafiz Bilal Ahmed, Sehrish Siddique, Jahangir Sarwar Khan, Jamal Nasir Malik
AFFLIATIONS:
Surgical Unit-1, Holy Family Hospital, Rawalpindi, Pakistan.
DOI: https://doi.org/10.36283/PJMD11-4/004
ORCID iD: 0000-0003-2168-1653
How to cite: Qureshi U, Ghazanfer R, Hasan SW, Ahmed HB, Siddique S, Khan JS, et al. Implications of Social Factors and Management Outcomes Among Patients with Corrosive Ingestion. Pak J Med Dent. 2022;11(4): 22-28. doi: 10.36283/PJMD11-4/
Background: Corrosive poisoning is a growing concern in developing countries and although management options have improved over the years, preventive strategies have failed to provide results. The objective of this study was to determine social and epidemiological factors related to corrosive intake in patients and to assess the effect of these factors on management outcomes in terms of morbidity and mortality.
Methods: A retrospective cross-sectional study was carried out in Surgical Unit-1 of Holy Family Hospital, Rawalpindi from February 2019 to June 2020. Each corrosive poisoning patient’s age, gender, residence, ethnicity, education, and financial status were recorded. Previous psychiatric illnesses were also recorded. Management outcomes in terms of wound infections, anastomotic leaks, weight gain, return to work and mortality were recorded. The correlation between social characteristics and the outcome of management was statistically analyzed using SPSS software.
Results: Out of 70 patients, the majority were females 48(68.6%). Chief suicidal motives included low-income [49(70%)], marital discord [16(22.5%)] and domestic violence [21(29.5%). Education level was the only social factor that was significantly associated with major as well as minor complications after intervention (p=0.021). Only 10(14.3%) patients had an established past psychiatric history. At 6 months follow-up, 57(81.4%) never went back to their original weight and only 22(31.4%) were able to return to work.
Conclusion: Domestic violence was found to be major cause of suicidal intent [21(29.5%)] followed by marital discord [16(22.5%)]. In managing such patients, a multidisciplinary approach including a surgical and gastroenterology team, psychologist and social workers must be employed.
Keywords: Corrosive; Demography; Epidemiology; Jejunostomy.
Global data show corrosive poisoning o be a grievous but often under-reported public health issue1. The term encompasses a wide range of immediate and long-term complications arising from intake of household or commercially available chemicals2. Sulfuric acids, nitric acid, hydrochloric acid, bleaches and alkalis like sodium or potassium hydroxide are the most common chemicals ingested.
Victims belong to both genders and all age groups. The causative factors vary from accidental ingestion to suicidal or homicidal attempts. The intent of self-harm can be present among 90 percent of the patients3,4. The mode of presentations can be extremely diverse. It usually depends upon the type of chemical ingested, the amount taken and its contact time with the aero digestive tract. Mild cases may only have oropharyngeal erythema and edema. Others may suffer from severe airway compromise and esophageal or gastric perforations. These can also present with massive bleeding and mediastinitis which is usually fatal5,6. Long-term problems usually include dysphagia due to a scarred and stenosed gastrointestinal tract. In addition to physical suffering, psychological morbidity is also profound.
In developing countries; fear of impeachment and social stigma bars most of the victims and their families from presenting to health care facilities. Those who do come get treated for medical problems only without any comprehensive assessment of the circumstances leading to such accidents5,7,8. This either results in incomplete treatment or the patient may repeat the act of corrosive intake resulting in drastic consequences. This study focused on the epidemiological characteristics of patients. We believed that identifying the vulnerable population will help in shaping better preventive strategies. The objective of this study was to determine social and epidemiological factors related to corrosive intake in patients presenting in a tertiary care setup and to assess the effect of these factors on management outcomes in terms of morbidity and mortality.
After approval from the institutional review board, a retrospective cross-sectional study was conducted in Department of Surgery Unit 1, at Holy Family Hospital from February 2019 to June 2020. All adult patients (n=70) with ages more than 15 and a history of corrosive poisoning presenting to the emergency department were included. Those referred from other health care facilities after first aid was also considered. Old cases and those already on follow-up in the upper GIT clinic were excluded. After written consent, a predesigned questionnaire was filled out for each patient at the time of presentation to an emergency.
Each patient’s demographic features like age, gender, residence, education, and financial status were recorded. A detailed history was taken to ascertain the type and amount of caustic taken along with events and reasons behind ingestion. History of any previous attempt or psychiatric illness was also taken. The intent of ingestion was determined after history taking and reviewing records of the medico-legal officer. The source of information was hospital records and telephonic conversations with the patient or attendants. Detailed physical examination including a primary survey was done to note injuries to aerodigestive tracts. Those needing high dependency care during the first 24 hours of admission were labeled as critical. According to departmental protocols, all patients underwent upper GI endoscopy on the morning after admission. Findings were recorded as per Zager’s classifications for tissue necrosis. During the hospital stay, patients were jointly reviewed by a team of gastroenterologists, surgeons and pulmonologists. Upon discharge, a psychiatric evaluation of all was done to diagnose and cure post ingestion depression. Weekly follow-ups were done in the upper GI clinic to ascertain the need for endoscopic dilatations, or other surgical interventions like feeding jejunostomies, gastrojejunostomies, or esophageal replacement surgeries. Co-relations of psychosocial factors were made with complications.
Complications were categorized as MAJOR and MINOR complications. wound infection, feeding tube blockage, basal atelectasis and post-op minor chest infections were categorized as MINOR complications while esophageal perforation during dilatation, anastomotic leakage, major chest infections, burst abdomen and feeding tube displacement with frank contamination were categorized as MAJOR complications
Data were analyzed using SPSS software for windows version 22. The quantitative data were described by mean ± standard deviation and qualitative variables were presented using frequency and percentage. The Chi-square test was used to assess the level of significance.
During the study period, a total number of 70 patients met the inclusion criteria. Out of these majority were females (n=48, 68.6%) belonging to the middle age group (average age 29.58 years). Patients from rural background (n=40, 57.1%) were slightly more than those from urban areas (n=30, 42.9%). The demographic details about marital status, education and financial status are mentioned in Table 1.
Table 1: Demographic characteristics of patients.
| Variables | Frequency n (%) | |||||
| Gender | Male | Female | ||||
| 22 (31.4%) | 48 (68.6%) | |||||
| Age Group | 15- 25 years | 26-30 years | >30 years | |||
| 28 (40%) | 23(32.9%) | 19(27%) | ||||
| Area | Rural | Urban | ||||
| 40 (57.1%) | 30 (42.9%) | |||||
| Marital Status | Married | Unmarried | ||||
| 39 (55.7%) | 31 (44.3%) | |||||
| Income (monthly) | <30,000 PKR | 30,000-100,000 PKR | >100,000 PKR | |||
| 48 (70.0%) | 19 (27.1%) | 3 (4.3%) | ||||
| Education Level | Traditional | Below Matric | Above Matric | |||
| 17 (24.3%) | 29 (41.4%) | 24 (34.3%) | ||||
| Profession | Unemployed | Housewives | Labour Class | Office Job | Forces | Teaching |
| 9 (12.67%) | 25 (35.2%) | 10 (14.08%) | 5 (7.04%) | 3 (4.3%) | 18(25.7%) | |
| Suicidal Intent | Marital Discord | Domestic Disputes/Violence | Sense of Failure in Life | Homicidal | By Mistake | |
| 16 (22.5%) | 21 (29.5%) | 9 (12.6%) | 8 (11.2%) | 16 (23.9%) | ||
| Source | Market Place | House Hold | Work Place | |||
| 33 (47.1%) | 30 (42.9%) | 7 (10.0%) | ||||
| Nature of Chemical Ingested | Commercial | Agricultural | Caustic | Bleach | ||
| 29 (41.4%) | 17 (22.9%) | 4 (7.1%) | 20 (28.6%) | |||
patients (n=38, 54.28%) presented directly to hospital emergency whereas 45.72% (n=32) were referred from secondary health care facilities after first aid. The mean time of presentation to the emergency department was 4.9±1.15 hours. Dysphagia (40%), pain (23%), shortness of breath (15%) and edema of lips plus oropharynx (12%) were the commonest presenting complaints. Patients (10%) presented in shock and needed resuscitation.
Patients (n=46) had themselves taken corrosive for the suicidal attempt. Out of 46 patients, 37 (80.43%) claimed this to be their first attempt. Only 10 patients (14.3%) had an established psychiatric history. Marital discord (n=16) and domestic violence (n=21) were chief suicidal motives. Characteristics of chemicals ingested along with their intent are mentioned in Table 1.
Out of 70 patients, 4 patients had major complications and 12 had minor complications. The mean difference between social factors with complications is given in Table 2. Although low income and marital disputes were related to complications statistically only the level of education was significantly associated with minor as well as major complications (p=0.021).
Table 2: Difference between social factors and complications.
| Variables | Characteristics | Complications | Total | Level of significance
(p-Value) |
|
| Major complications | Minor Complications | ||||
| Cause of Poisoning | Marital discord | 2 | 1 | 3 | 0.130 |
| Domestic disputes | 0 | 5 | 5 | ||
| Career/educational setbacks | 1 | 1 | 2 | ||
| Homicidal | 1 | 1 | 2 | ||
| Accidental | 0 | 4 | 4 | ||
| Gender | Male | 1 | 4 | 5 | 1.000 |
| Female | 3 | 8 | 11 | ||
| Age Group | 15-25 | 4 | 6 | 10 | 0.202 |
| 26-30 | 0 | 3 | 3 | ||
| >30 | 0 | 3 | 3 | ||
| Income | <30,000 PKR | 3 | 12 | 15 | 0.250 |
| >100,000 | 1 | 0 | 1 | ||
| Education | Traditional | 0 | 5 | 5 | 0.021 |
| Matriculation | 2 | 7 | 9 | ||
| Above Matric | 2 | 0 | 2 | ||
| Marital Status | Married | 3 | 5 | 8 | 0.569 |
| Unmarried | 1 | 7 | 8 | ||
Endoscopy was performed on all patients within 24 hours. Endoscopic findings were reported according to standard Zagar staging which is explained in detail in the chart below. The esophagus was found to be the commonest affected site. 64.3% of patients had to undergo more than one dilatation. Patients (33) improved on dilatations alone, and 37 were offered surgical intervention. Thus, 7 out of this refused treatment furthermore, 16 feeding jejunostomies, 10 gastrojejunostomies and 4 esophageal replacement surgeries were done. Details of the grade and location of injury are given in Figures 1 and 2. For those undergoing surgery mean hospital stay was calculated. Those who underwent feeding jejunostomy on average had to stay 4.5+/- 2.1 days. Whereas, in cases of gastrojejunostomies and esophagectomies it was 14+/- 3.9 days.
At 6 months follow-up patients were inquired about quality-of-life post-ingestion. N=62(88.6%) said it affected their lifestyle, and 81.4% (n=57) never went back to their original weight. Only 31.4% (n=22) were able to return to work within 6 months.
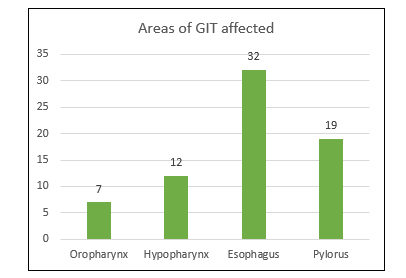
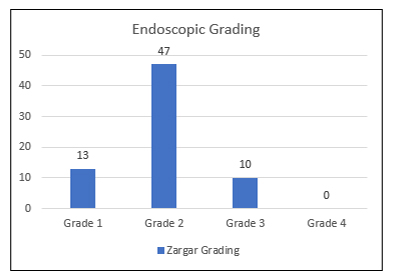
Figure 1: Chart showing areas of GIT primarily affected by Corrosive.
Figure 2: Chart showing endoscopic grading of severity of damage by Corrosive.
In the current study, the main social factor that is significantly associated with morbidity and complications is “education” (p-value 0.021). Although most of our study population had an education level below matriculation, this was independently associated with worse outcomes. Although low income and “suicidal intent” of poisoning were associated with major as well as minor complications after surgery, they failed to reach statistical significance (p-value of 0.250 and 0.130 respectively). This study thus shows the importance of awareness and education as the sole predictor of prognosis after corrosive intake.
In the study, most of the patients belonged to the younger age group. The mean age was found to be 28.73±14.14 years for males and 30.23±12.18 for females. These figures tally with another indigenous study3. The age of the victim is an important factor. Different age groups have their causes of exposure to such chemicals. In developed countries, corrosive ingestion makes up for almost one-third of all reported cases of poisoning8. The situation is even worse in third-world countries. At this point, the lack of poison control committees and social taboos make the bulk of the problem almost unfathomable. According to the WHO report on developing Asian countries, only 37 papers were written about corrosive poison over 17 years. Woefully only 7 of these dealt with an epidemiological aspect of the problem9,10. A recent audit published by the thoracic surgery department at Nishtar Medical University, Multan showed corrosive poisoning to be the leading cause of admission (49.8%). Corrosive-related upper GIT endoscopies also topped the procedures list (38.7%) 11.
Globally children are found to be the commonest sufferers12. Natural curiosity, lack of understanding and playful nature are the commonest undergoing factors. In the USA more than 80% of cases are reported in the pediatric population8. However, in different countries incidence may vary greatly among various age groups. A 2017 Taiwanese study showed that 65% of the victims were more than 40 years old. Twenty-two percent among these were above 65 years of age13.
Pakistan, with its 45% population younger than 40 years of age, depends heavily on its youth for economical and developmental activities14. Seeing the younger generation to be the worst afflicted by this problem is sobering. This study found that among patients with ages less than 40 years (n= 60), 65% (n=39) had suicidal intent and 40% (n=24) gave a positive history of psychiatric disorder. These grim facts raise serious questions about our youth’s mental health and social satisfaction levels15.
The female tendency for corrosive ingestion is well established and remains undisputed nationally and internationally16,17. A 2012 study in Macedonia reported ratio of females and males is 2.5:1. A Taiwanese study also reported sex-specific incidence of corrosive injury to be significantly higher in females4,13. In this study 55% of patients were women. Most of them were married, housewives and belonged to lower socioeconomic status and 33% had a rural background. Suicidal intent was positive in many cases (51.9%). Domestic abuse and marital discords were commonest reported motives. A 2018 study by Hashmi et al. in Multan presented similar statistics. They opined that these were due to a social structure where unhappy and oppressed women resorted to self-poisoning while trying to escape from the hardships of life3.
Most of the women ingested household cleaning chemicals like toilet cleaners, laundry detergents and bleaches. These potentially harmful substances are easily available as over-the-counter products in most third-world countries. Women being the chief caretakers of the house have easy access to them. This might tempt them to use these as an easy way-out during periods of emotional stress. Identification of vulnerable portions of society and strict legislation about the availability of such products can help diminish this alarming trend among females2,3. Information about the actual chemical composition of corrosives ingested might be very useful for emergency physicians in initiating a timely and targeted therapy. Acids cause coagulative and alkalis to cause liquefactive necrosis. Each has its spectrum of injuries5,6. This study tried to meaningfully classify commonly ingested corrosive substances based on their chemical constituents. This was however futile and most of the victims and their families were unaware of the exact nature of the substance ingested. Container labels when brought to the hospitals had woefully inadequate information to offer. The majority showed only trade names with no details about the composition and strengths of constituents. Eventually, the substances were classified into 4 broad categories depending upon the area of their usage.
Patients were also questioned about how they came across these chemicals, 42.9% reported that they were already present at home whereas 47.1 % claimed to have purchased them from the market. This easy access to such potentially dangerous substances is a sobering thought. A 2020 study showed that strict legislation alone can effectively limit the number of such unfortunate events quite effectively18-20.
Emergency endoscopy within 24 hours of the presentation was performed in all patients as a part of hospital protocol. Since 13 had mild erythema (Zagar 1), 47% had a haemorrhage, erosions and focal ulcers (Zagar 2) while 11 had deep ulcers (Zagar grade 3) warranting ICU admission and surgical intervention. A 2015 study from Military Hospital Rawalpindi also found most corrosive injuries to be of a higher grade on endoscopic examination (24% grade 2, 46% grade 3)19. Patients with high-grade injury on initial endoscopy tend to have progressively higher rates of stricture formation20-22.
Patients (64.3%) had to undergo more than one dilatation, 16 feeding jejunostomies, 10 gastrojejunostomies and 4 esophageal replacement surgeries were done. The average stay for those undergoing minor and major interventions was almost one and two weeks respectively. On 6 monthly follow up 88.6% of patients admitted that the incident permanently prevented them from returning to their normal lifestyle. Identification of the population most vulnerable to this type of poisoning and the causative factors behind ingestion are important23-25. Regulatory and law enforcement agencies can then take practical measures to discourage this trend. Understanding the clinical presentation and further course after corrosive poisoning can also aid health care workers in better managing these emergencies.
Management of corrosive poisoning is a multidisciplinary activity and is incomplete without addressing socioeconomic and psychological factors leading to it and responsible for aggravating or adversely affecting it. In managing such cases, social workers, psychologists, and stakeholders in government bodies should also be involved.
The authors would like to acknowledge the hospital administrative staff for helping them in retrieving the files of all the participating patients. They would also like to acknowledge the Gastroenterology Department of the Holy Family Hospital, Rawalpindi for coordinating with them and providing the data on non-operated patients.
The authors declared no conflict of interest.
The authors declared no conflict of interest.
This study has been approved by the “Institutional research and ethics forum” of Rawalpindi medical university after its presentation to the institutional review board. Approval letter attached for reference (Ref. no: 218/IREF/RMU/2022).
The consent of the patients was taken before adding them to the study.
UQ generated the research question and the whole concept of the research was designed. RG did the data analysis and results. SWH reviewed the article and presented it to various institutional committees for approval and made necessary changes to the article. SWH was also the corresponding author. HBA designed the proforma and had a major role in data collection. SS reviewed the article and made the necessary corrections. JSK did the final proofreading and analysis. JNM contributed to data collection.
UQ generated the research question and the whole concept of the research was designed. RG did the data analysis and results. SWH reviewed the article and presented it to various institutional committees for approval and made necessary changes to the article. SWH was also the corresponding author. HBA designed the proforma and had a major role in data collection. SS reviewed the article and made the necessary corrections. JSK did the final proofreading and analysis. JNM contributed to data collection.
- Tustumi F, da Costa Seguro FC, Szachnowicz S, Bianchi ET, Morrell AL, da Silva MO, et al. Surgical management of esophageal stenosis due to ingestion of corrosive substances. J Surg Res. 2021;264:249-259. doi: 10.1016/j.jss.2021.03.009
- Kalayarasan R, Ananthakrishnan N, Kate V. Corrosive ingestion. Indian J Crit Care Med. 2019; 23(Suppl 4): S282-S286. doi: 10.5005/jp-journals-10071-23305
- Hashmi MU, Ali M, Ullah K, Aleem A, Khan IH. Clinico-epidemiological characteristics of corrosive ingestion: a cross-sectional study at a tertiary care hospital of Multan, South-Punjab Pakistan. Cureus. 2018;10(5):1-10. doi: 10.7759/cureus.2704
- Chibishev A, Pereska Z, Chibisheva V, Simonovska N. Corrosive poisonings in adults. Mater Sociomed. 2012;24(2):125-130. doi: 10.5455/msm.2012.24.125-130
- Bharath Kumar C, Chowdhury SD, Ghatak SK, Sreekar D, Kurien RT, David D, et al. Immediate and long-term outcome of corrosive ingestion. Indian J Gastroenterol. 2019;38(4):356-361. doi: 10.1007/s12664-019-00978-z
- Singh AN, Kilambi R, Madhusudhan KS, Pal S. An alternative approach to life-threatening gastrointestinal bleeding after corrosive ingestion. Indian J Surg. 2018;80(2):187-189. doi: 10.1007/s12262-018-1739-y
- Güney C, Coskun A. Examination of demographic characteristics of drug and corrosive poisonings, morbidity and mortality in children in terms of emergency department and pediatric surgery. Preprints. 2020:1-17. doi: 10.20944/preprints202002.0154.v1
- Hall AH, Jacquemin D, Henny D, Mathieu L, Josset P, Meyer B. Corrosive substances ingestion: a review. Crit Rev Toxicol. 2019;49(8):637-669. doi: 10.1080/10408444.2019.1707773
- Bielecki JE, Gupta V. Caustic Ingestions. StatPearls [Internet]. 2020. Available from: https://europepmc.org/article/nbk/nbk557442
- Contini S, Swarray-Deen A, Scarpignato C. Oesophageal corrosive injuries in children: a forgotten social and health challenge in developing countries. Bull World Health Organ. 2009;87:950-954. doi: 10.2471/BLT.08.058065
- Ullah MK, Hashmi MU, Sarwar M, Khan AA, Khan IH. Surgical audit: A process of self-evaluation for better future. Prof Med J. 2020;27(05):1049-1053. doi: 10.29309/TPMJ/2020.27.05.4208
- Lakshmi CP, Vijayahari R, Kate V, Ananthakrishnan N. A hospital-based epidemiological study of corrosive alimentary injuries with particular reference to the Indian experience. Natl Med J India. 2013;26(1):31-36.
- Chen CM, Chung YC, Tsai LH, Tung YC, Lee HM, Lin ML, et al. A nationwide population-based study of corrosive ingestion in Taiwan: incidence, gender differences, and mortality. Gastroenterol Res Pract. 2016;2016:1-8. doi: 10.1155/2016/7905425
- Khalid A, Asad AZ. Social entrepreneurship is one of the way forward to youth empowerment in Pakistan. Pak Vis. 2019;20(1):1-7.
- Urooj I, Javed I, Ahmad S. Intentions to Urban Migration among Youth: A Case of district Khushab of Pakistan. J Econ Impact. 2020;2(1):24-36. doi: 10.52223/jei0201204.
- Munema Khan MK, Raza S. Gender based differences in patients of poisoning managed at a Medical Unit. J Pak Med Assoc. 2019;69(7):1025-1028.
- Ain QU, Jamil M, Safian HA, Akhter TS, Batool S, Arshad M, et al. Assessing the degree of acute esophageal injury secondary to corrosive intake: Insights from a public sector hospitals of a developing country. Cureus. 2020;12(10):1-6. doi: 10.7759/cureus.10858
- Cvetković D, Živković V, Nikolić S. Lesser availability of corrosive substances could decrease the rate of suicide attempts and corrosive attacks over time. Forensic Sci Med Pathol. 2020;16(3):567-568. doi: 10.1007/s12024-020-00264-x
- Ahsan O, Razzaq K, Abbas W, Zarrin F. Caustic ingestion injuries-at military hospital rawalpindi. Pak Armed Forces Med J. 2015;65(2):221-225.
- Shahzad A. Relationship of Esophageal Strictures with Esophageal Injury after Corrosive Intake. J Rawalpindi Med Coll. 2016;20(4):254-257.
- Jones MM, Benrubi ID. Poison politics: a contentious history of consumer protection against dangerous household chemicals in the United States. Am J Public Health. 2013; 103(5): 801-812. doi: 10.2105/AJPH.2012.301066
- Özkan EA. Evaluation of poisoning cases admitted to the pediatric emergency clinic retrospectively. J Exp Clin Med. 2022;39(1):199-203.
- Badsar A, Taramsari MR, Attarchi M, Kojidi HM, Maleknejad S, et al. Investigating the predictive factors of gastrointestinal lesions due to consumption of household sodium hypochlorite in pediatric and adult Rasht referral hospitals. J Curr Oncol Med Sci. 2022;2(1):153-159.
- Varshney VK, Nayar R, Balakrishnan S, Birda CL. Robotic Ivor-Lewis Esophagectomy for corrosive-induced esophageal stricture. Cureus. 2022;14(4):1-6. doi:10.7759/cureus.23738
- Chen RJ, O’Malley RN, Salzman M. Updates on the Evaluation and Management of Caustic Exposures. Emerg Med Clin. 2022;40(2):343-364. doi: 10.1016/j.emc.2022.01.013
This is an open-access article distributed under the terms of the CreativeCommons Attribution License (CC BY) 4.0 https://creativecommons.org/licenses/by/4.0/