By Naila Parveen1, Saima Athar2, Lubna Riaz3, Ikhlas Ahmed4, Kainat Sattar Shaikh4, Mahnoor Channa4
AFFLIATIONS:
- Department of Physiology, Liaquat National Medical College, Karachi, Pakistan.
- Department of Anatomy, Liaquat National Medical College, Karachi, Pakistan.
- Department of Forensic Medicine, Dow Medical College, Dow University of Health Sciences, Karachi, Pakistan.
- Student, Liaquat National Medical College, Karachi, Pakistan.
Background: The rapid transmission of corona virus from symptomatic as well as non-symptomatic subjects has caused a serious health crisis globally. The Ministry of health, to curb this lethal pandemic, has imposed various standard operating procedures to minimize its spread. Amongst them, avoiding close contact with others limits the spread of Covid-19 and reduces the risk of infection. The study aimed to compare barriers and motivators of social distancing practices among undergraduate male and female students during Covid-19 pandemic.
Methods: This cross-sectional study was conducted at Liaquat National Hospital and Medical College from November 2020 until December 2020. The undergraduate medical students (n=303) participated in the study. The questionnaires regarding barriers and motivators of social distancing were uploaded via Google forms to be filled by the participants. Chi squared test was applied for analysis among the variables and p value ≤0.05 was taken statistically significant.
Results: The study showed social distancing motivators which included, social responsibility 174(57.5%), protecting sense for others in order to save them from getting sick 115(38%), and personal protection 126(41.5%). The current study reported that public lockdowns superimposed by the Government also accounted for social distancing 44(14.5%). Comparison of motivators of social distancing among gender was found to be statistically significant (p-value <0.05). However, insignificant comparison of barriers was found among genders (p=0.151).
Conclusion: Social responsibility factor was sufficiently same in both the genders (p=0.01). However, self- protection was the major motivator for practicing social distancing among female participants of the study when compared with males.
Keywords: Social Distancing; Covid 19; Pandemic; Social Responsibility.
The first active case of corona virus reported in Wuhan, China in December, 2019, has turned into a pandemic disease with various economic and psychosocial impact and a need for behavioral pattern changes in order to prevent the spread of the disease1,2. The seriousness of the impact of this pandemic and increase in the mortality rate has forced many countries to intervene and impose restrictions such as lockdowns, closure of all educational institutes and offices, recreational centers, public places and an urge to work from home3.
Moreover, it was mandatory for the public to follow various preventive tools such as wearing facemasks, avoiding social gatherings and disinfection by use of hand sanitizers and anti-septic solutions. In order to attain minimal interaction amongst individuals, social or physical distancing policies have come into existence for practical implications at both national and international levels4.
A number of studies have identified that the spread of this covid-19 virus occurs either from individuals having the symptoms and those even without the symptoms. These asymptomatic people represent as carriers of the disease5-7. According to researchers, transmission of this virus is much more rapid as compared to the influenza flu virus8,9. In order to minimize the overwhelming burden on health care resources, various models implicated for preventing the transmission of covid-19 has supported the fact that adherence to social distancing measures can flatten the curve and can play a tremendous role in the spread of this pandemic10.
A recent survey has identified multiple barriers and motivators regarding practicing of social distancing. According to their analysis, structural barriers such as family norms, nature of work and social and religious obligations hindered most of the individuals to practice social distancing. Psychological effects such as anxiety and depression also prevented them from practicing social distancing. The factors that motivated people to practice more social distancing included self protection from covid-19 and interacting with others through social media rather than physically11. The purpose of this study was to motivate people to continue practicing social distancing and reduce the spread of this corona virus infection. Thus, by identifying the barriers and comparing the motivators of social distancing practices among the gender during Covid-19 pandemic, effective adherence to social distancing can be possible.
We conducted this cross-sectional study at Liaquat National Hospital and Medical College Karachi, after approval by the institutional review board and research and ethics committee. Sample size was calculated using OpenEpi-sample size calculator with reported prevalence of social distancing as P= 26.9% 12, CI= 95%. The duration of study was from October 2, 2020 until December 2, 2020.
Three hundred and three undergraduate medical students of MBBS participated in the study through convenience sampling technique. Medical students of MBBS, both genders in the age range of 18-25 years filled the questionnaire regarding barriers and motivators of social distancing send to them via Google forms. A total of two months was required to complete this research project. Inclusion criteria included both male and female medical students irrespective of the medical year of MBBS of Liaquat National Hospital and Medical College willing to participate in the study, with age ≥18years or ≤25 years. Students not willing to participate or those with incomplete Google forms were excluded from the study. Statistical analysis was done by SPSS. Chi square test (X2) was applied for analysis among the variables and p value ≤0.05 was taken as statistically significant.
Mean age calculated was 22±2.06 years. Male and female students who participated in the study were 35% and 65% respectively. Responses to different variables regarding social distancing information, barriers and motivators presented as percentage frequencies. Around 100% of the students responded to the meaning of social distancing and 84.9% were currently practicing social distancing. 78.2 % of the responses were of the opinion that social distancing practices decreases the risk of infection and 31.4% of the students found it to be very effective for them. Student’s response for the structural barriers included nature of work (33.3%), family norms (29.8%), religious obligations (23.7%) and peer pressures (13.2%) as in Figure 1.
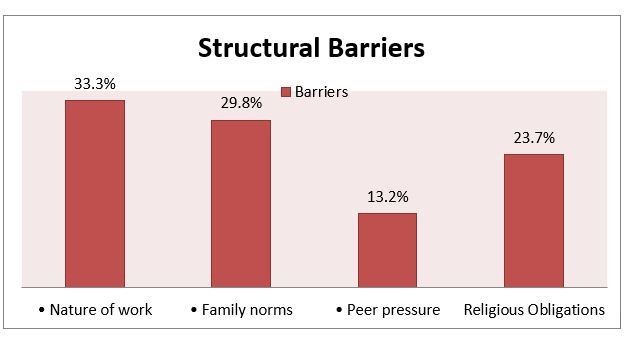
Figure 1: Structural barriers of social distancing.
Moreover, 66.4% of the participants were of the opinion that practicing social distancing was responsible for the deterioration of mental health and 58% believed that it resulted in boredom.
On comparison of motivators among gender, we found that that the males were more socially responsible and they wanted to maintain social distance for protecting others as compared to females. However, females were more cautious for their health and implemented social distancing to protect themselves from the disease as compared to males (p value: 0.016) as in Table 1.
Table 1: Comparison of motivators for social distancing among gender.
| Gender | Total
Frequency n (%) |
Motivators | p-Value | |||
| Social responsibility
n (%) |
Others protection
n (%) |
Personal protection
n (%) |
Lockdown
n (%) |
|||
| Males | 106(35.0) | 55(51.8) | 32(30.1) | 11(10.3) | 08(7.5) | 0.016* |
| Females | 197(65.0) | 60(30.4) | 44(22.3) | 72(36.5) | 21(10.6) | |
*p value ≤0.05 was taken as significant, p value obtained by Chi square test (X2).
Insignificant statistical difference was found among gender and structural barriers. However, males found that religious obligations were their main barrier and according to females, family norms prevented them from practicing social distancing during the pandemic (Table 2).
Table 2: Comparison of structural barriers for social distancing among gender.
| Gender | Total
Frequency n (%) |
Family norms
n (%) |
Peer pressure
n (%) |
Nature of work
n (%) |
Religious obligations
n (%) |
p– Value |
| Male | 106(35.0) | 26(24.3) | 14(13.5) | 29(27.0) | 37(35.1) | 0.151 |
| Females | 197(65.0) | 66(32.9) | 39(20.0) | 60(30.6) | 32(16.5) |
*p value ≤0.05 was taken as significant, p value obtained by Chi square test (X2).
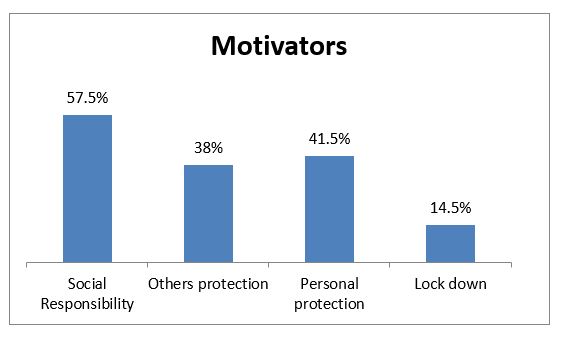
Figure 2: Motivators of social distancing.
In view of the fact that the pandemic, strict measures imposed for adherence to social distancing across the globe to restrict its rapid spread. This has led to major changes in the lifestyle of the general population, which has either facilitated or prevented them to continue practicing social distancing. Early interventions by the public health can help individuals to adhere to these preventive health behaviors in the end.
In this study, we determined various factors that prevented adherence to social distancing and those that facilitated it. Among the structural barriers, around 33.3% of the participants marked nature of work (self employed and organizational level barriers) as the key factor that prevented from practicing social distancing. This was in agreement with the study conducted by Coroiu et al. They found that organizational level barriers such as “my work cannot be done remotely” (16%) and “my workplace requires me to come into work” (11%) prevented from adherence to social distancing13.
Besides work nature, family norms such as marriages and condolences also accounted for 29.8% prevention from practicing of social distancing. Religious gatherings as a barrier were spotted by 23.7% of the participants. These results were supported by Rehman et al. study that depicted mass gatherings as a major barrier for effective social distancing and Escher who conducted a study in 2020 stating that how religious and social gatherings are making life harder for the governments to tackle the disease14,15.
Moreover, boredom and mental health deterioration was accounted as barriers by 58% and 66.4% respectively. Wirz et al. and Coroiou et al. reported similar findings in their study. They analyzed that fear of mental health deterioration prevented most of the individuals from practicing social distancing11,13. Another research conducted by Williams et al. in UK which was in concord with the current study, analyzed that most of the participants had a negative perception of social distancing and isolation during the pandemic due to its immense impact on their psychological and social well-being16.
According to self-determination theory, there are two types of motivations; intrinsic and extrinsic motivations. Intrinsic motivation relates to the notion where the individual derives pleasure from the behavior, and extrinsic motivation, where external pressures are facilitating adherence to behaviour17. Practicing social distancing at an individual level would benefit the entire society i.e.; social responsibility represented 57.5% as the most frequently endorsed motivator to engage in social distancing in our study. This was in concordant with Coroiu et al. study, in which 84% of the participants were of the opinion” I feel a sense of responsibility to protect our community”. Waselewski et al. found evidence in their survey that people believing covid-19 as the biggest threat to the society in our time had an intent to practice more social distancing13,18.
In the present study, another motivator to comply with social distancing (“Not wanting others to get sick”) was opted by 27.7% of the participants. This was in favor with the online experiment conducted by Lunn et al. whose findings suggested that the thought of infecting vulnerable people or large numbers of people motivated most of the participants to practice social distancing more19. Moreover, Charles et al. also addressed in their study that favorable attitude was found among individuals who strongly believed that strict compliance to social distancing measures would reduce the transmission of this deadly Covid infection20.
Regarding social media as one of the motivators for social distancing, majority of the students considered WhatsApp as the major source for social contact and an inspiration for physical distancing. This was in contrast with Wirz et al. who reported Facebook as the best source to reach individuals who are engaged in social distancing11. In our study, we found that in males, social responsibility was the major motivator for most of the individuals to practice social distancing. This was in contrast with the study conducted by Coroiu et al. However, females in our study opted for protecting self as the motivator to continue practicing social distancing and this too was consistent with the Coroiu et al. and Pedersen et al. study. They reported that females found self-protection as the strongest facilitator in their adherence to social distancing practice and that differed significantly on comparison with male participants13, 21.
Other studies by Mohammadpour et al. and Galasso et al. which was consistent with our findings, too predicted that regarding self-care behaviors, women were more compliant to social distancing practices and were more likely to observe social distancing than men22,23. Paykani et al. also proposed the same findings in their study in Tehran24. In addition, Oosterhoff et al. conducted a study in the United States and found that greater than 60% of young population declared that the motivator, which facilitated them best to engage in social distancing practices, was their social responsibility and not wanting others to get the disease, supported this. Keeping this in view, there is an urgent need to review our public policies and that early health care intervention would likely help in the prevention of the spread of this pandemic25.
The most significant factor that motivated the male students to practice more social distancing was their social responsibility and not wanting others to get sick. Self-protection was the major motivator to continue practicing social distancing in females. There was no statistical significant difference on comparison of various structural barriers for social distancing among gender.
We would like to acknowledge Dr. Shireen Jawed for her immense contribution.
Authors declared no conflict of interest.
Institutional Ethical Review Committee of Liaquat National hospital approved the study (Ref: App#0584-2020 LNH-ERC.)
Online consents of students were obtained.
NP had given the conception, design and write-up. SA did the data analysis and interpretation. LR drafted the article and revising it critically for important intellectual content. IA performed the data collection and literature search. KSS and MC also assisted in the data collection procedures and data entry in the SPSS.
- Galea S, Merchant RM, Lurie N. The mental health consequences of COVID-19 and physical distancing: the need for prevention and early intervention. JAMA Intern Med.2020; 180(6):817-818.
- World Health Organization. Pneumonia of unknown cause–China (Cited on: 14-3-2021). Availablefrom: https://www.who.int/csr/don/05-january-2020-pneumonia-of-unkown-causechina/en/
- Koh WC, Naing L, Wong J. Estimating the impact of physical distancing measures in containing COVID-19: an empirical analysis. Int J Infect Dis. 2020; 100:42-49.
- Chu DK, Akl EA, Duda S, Solo K, Yaacoub S, Schünemann HJ, et al. Physical distancing, face masks, and eye protection to prevent person-to-person transmission of SARS-CoV-2 and COVID-19: a systematic review and meta-analysis. Lancet. 2020; 395: 1973-1987.
- Bai Y, Yao L, Wei T, Tian F, Jin DY, Chen L, et al. Presumed asymptomatic carrier transmission of COVID-19. JAMA. 2020;323(14):1406-1407.
- Guan WJ, Ni ZY, Hu Y, Liang WH, Ou CQ, He JX, et al. China medical treatment expert group for Covid-19. Clinical Characteristics of Coronavirus Disease 2019 in China. N Engl J Med. 2020;382(18):1708-1720.
- Rothe C, Schunk M, Sothmann P, Bretzel G, Froeschl G, Wallrauch C, et al. Transmission of 2019-nCoV infection from an asymptomatic contact in Germany. N Engl J Med. 2020;382(10):970-971.
- Inglesby TV. Public health measures and the reproduction number of SARS-CoV-2. JAMA. 2020;323(21):2186-2187.
- Pan A, Liu L, Wang C, Guo H, Hao X, Wang Q, et al. Association of public health interventions with the epidemiology of the COVID-19 outbreak in Wuhan, China. JAMA. 2020;323(19):1915-1923.
- Eubank S, Eckstrand I, Lewis B, Venkatramanan S, Marathe M, Barrett CL. Commentary on Ferguson, et al., “Impact of non-pharmaceutical interventions (NPIs) to reduce COVID-19 mortality and healthcare demand”. Bull Math Biol. 2020;82(4):1-7.
- Wirz CD, Schwakopf JM, Brossard D, Brown LD, Brauer M. Self-reported compliance and attitudes about social distancing during the COVID-19 outbreak. OSF Preprints. 2020;10:1-6.
- Thunström L, Newbold SC, Finnoff D, Ashworth M, Shogren JF. The benefits and costs of using social distancing to flatten the curve for COVID-19. J Benefit Cost Anal. 2020;11(2):179-95.
- Coroiu A, Moran C, Campbell T, Geller AC. Barriers and facilitators of adherence to social distancing recommendations during COVID-19 among a large international sample of adults. PLoS One. 2020;15(10):1-20.
- Escher Jr AR. An ounce of prevention: coronavirus (COVID-19) and mass gatherings. Cureus. 2020; 12(3):1-3.
- Rehman IU, Khan HR, Zainab WE, Ahmed A, Ishaq MD, Ullah I. Barriers in social distancing during Covid19 pandemic – is a message for forced lockdown? J Med Res Innov. 2020;4 (2):1-2.
- Williams SN, Armitage CJ, Tampe T, Dienes K. Public perceptions and experiences of social distancing and social isolation during the COVID-19 pandemic: a UK-based focus group study. BMJ Open. 2020; 10(7):1-8.
- Ryan RM, Deci EL. Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being. Am Psychol. 2000;55(1):68-78.
- Waselewski E, Waselewski M, Harper C, Dickey S, Bell SA, Chang T. Perspectives of US youth during initial month of the COVID-19 pandemic. Ann Fam Med. 2021;19(2):141-147.
- Lunn PD, Timmons S, Belton CA, Barjaková M, Julienne H, Lavin C. Motivating social distancing during the COVID-19 pandemic: An online experiment. Soc Sci Med. 2020;265:1-7.
- Charles G, Jain M, Caplan Y, Kemp H, Keisler A, Sgaier S. Increasing uptake of social distancing during COVID-19: behavioral drivers and barriers among US population segments. SSRN Electron J. 2020:1-43.
- Pedersen MJ, Favero N. Social distancing during the COVID-19 pandemic: who are the present and future noncompliers? Public Admin Rev. 2020;80(5):805-814.
- Mohammadpour M, Ghorbani V, Khoramnia S, Ahmadi SM, Ghvami M, Maleki M. Anxiety, self-compassion, gender differences and COVID-19: predicting self-care behaviors and fear of COVID-19 based on anxiety and self-compassion with an emphasis on gender differences. Iran J Psychiatry. 2020;15(3):213-219.
- Galasso V, Pons V, Profeta P, Becher M, Brouard S, Foucault M. Gender differences in COVID-19 attitudes and behavior: Panel evidence from eight countries. Proc Natl Acad Sci USA. 2020 ;117(44):27285-27291.
- Paykani T, Zimet GD, Esmaeili R, Khajedaluee AR, Khajedaluee M. Perceived social support and compliance with stay-at-home orders during the COVID-19 outbreak: evidence from Iran. BMC Public Health. 2020; 20(1):1-9.
- Oosterhoff B, Palmer CA, Wilson J, Shook N. Adolescents’ motivations to engage in social distancing during the COVID-19 pandemic: associations with mental and social health. J Adolesc Health. 2020;67(2):179-185.
This is an open-access article distributed under the terms of the CreativeCommons Attribution License (CC BY) 4.0 https://creativecommons.org/licenses/by/4.0/